8
Tooth Wear and Other Signs of Ageing
8.1 Introduction
Tooth wear is the progressive loss of enamel and exposed cementum and dentine because of frictional contact between teeth and contact between teeth and the food or foreign bodies. Tooth wear is a complex process, and the rate of loss is difficult to predict;260 teeth may wear prematurely or as part of ageing. Each contact of a tooth with its antagonists, food, etc. results in the loss of a few nanometres of the tooth surface, which over time results in a marked loss of tissue.205 Determinants of wear include: hardness, size and shape of the food particles, the pH of the food, friction and intensity of the compressive force, the force direction, and the amount and nature of the saliva.260
8.2 Ageing
8.2.1 Enamel
Enamel wear increases with age and its permeability changes due to the uptake of ions from the environment. In forensic science and anthropology age is estimated of degree of wear and signs of ageing of dentine.120 218
8.2.2 Dentine
The mineralisation and hardness of dentine increase while tubular diameter decreases with age. Empty tubules are the result of peripheral irritation and form opaque areas called dead tracts. Normally, the tubules scatter light, but sclerosis, i.e. the deposition of minerals within the tubules lying underneath slow, destructive lesions caused by external stimuli, minimises the light refraction and makes the dentinal areas translucent.347 The increase in translucency of the apical part of the tooth23 is a physiological age change,120 which ultimately can extend over two-thirds of the root. Predentine and odontoblasts are absent underneath in these areas.328 348 The correlation between root translucency and age varies by tooth type, from 0.55 (mandibular central incisor) to 0.83 (first molar roots).22 A larger part of the root becomes transparent in Caucasians than in Malaysians and Chinese.394 The length of the translucent part as a percentage of the root length is a slightly better determinant of age. The correlation was very low (r = 0.08) in a sample of teeth from the nineteenth century, because filiform structures (fungal, bacterial?) lying along the paths of the tubules caused a chalky root appearance.327
After death, the organic component, particularly in dentine, disintegrates. The enamel is then easily removed, like removing as a cap from over the opaque, chalky and brittle crown dentine. Wet earth and mummification delay disintegration.172 Further, the enamel of teeth stored under dry conditions for a long time becomes brittle.
The intensity of the dentinal (and cemental) fluorescence under green light increases linearly with age.176
8.2.3 Pulp
Secondary Dentine
After eruption, 0.5 µm68 of physiological secondary dentine is formed daily, which leads to narrowing of the pulp cavity; in posterior teeth this occurs disproportionately at the floor and roof of the pulp chamber. The mean pulp length (10–12 mm) in elderly people is about 7 mm less than in young adults. The mesiodistal pulp width at the cervix decreases from 1.1–1.4 mm to 0.2–0.3 mm.233 The deposition of fibro-dentine also reduces the pulp space in maxillary and mandibular canines, but not before the age of 60 years; there is greater reduction in the size of the pulp cavities in the incisors.269 318 The tubules bend at the junction between the primary and secondary dentine. Secondary dentine (and cementum) is also formed in retained (unerupted) teeth.247
Tertiary Dentine
External stimuli induce the formation of tertiary dentine (Chapter 5), in general with few and irregular tubules,317 but tertiary dentine is a poor barrier to ingress of bacteria and bacterial toxins.362
Ivanovic et al. found that within 3 months, the largest amount of tertiary dentine was formed underneath a lining of calcium hydroxide, a smaller amount underneath Ledermix, and the smallest under zinc oxide eugenol. Thereafter, the daily rates of tertiary dentine production were similar.146 Others have found no difference, after 5 and 8 weeks, in the thickness of tertiary dentine underneath calcium hydroxide and zinc oxide eugenol.68
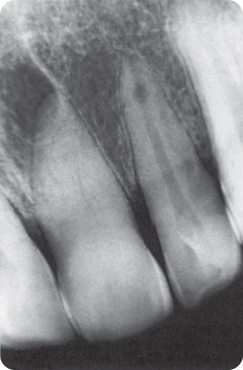
Deposition of tertiary dentine leads to obliteration of the pulp cavity (Figure 8.1); in older persons tertiary dentine is laid down in response to chronic stimuli and, in young persons, to a single strong (traumatic) stimulus. Pulps that appear to be obliterated on radiographs are often vital (90% in one study).300
Figure 8.1 The pulp cavity of the (caries-free) central incisor is almost totally obliterated after an accident.
Denticles and Pulp Stones
Calcified structures in the pulp (Figure 8.2) are more common in older than younger persons.132 288 Such denticles are found throughout the dentition in both anomalous (dentine dysplasia, see Chapter 3) and healthy teeth, and are attached to the pulpal walls or are free floating within the pulp. They are classified as true or false denticles and diffuse calcification of the pulp.212 288 329 367 372
- True denticles are mainly found in the pulp chamber and may occupy almost the entire pulpal space. They consist of an organic matrix and dentinal tubules. True denticles may be present in teeth that are non-functional, for example due to lack of contact with an antagonist.
- False denticles, called pulp stones, are found within the pulp chamber and the root canal. They consist of concentric or lamellar layers, which probably consist of calcified, degenerated pulp tissue. Heavy masticatory forces are associated with an increase in the number of pulp stones.
- Diffuse calcifications147 occur along the long axis of the radicular pulp and are associated with the pulpal blood vessels or collagen fibrils.
Figure 8.2 Radiograph showing a pulp stone in the pulp chamber of the maxillary first molar.

In an Indian study, 3% of deciduous incisors and about 25% of second molars showed diffuse calcifications.175 About 20% of the teeth of a sample of Iraqi 13–14-year-olds and 20–40-year-old Israelis contained denticles; Israeli women were more likely to have denticles than men.22 360 “Pulp stones” are present in all tooth types, regardless of eruptive status. Blood chemistry, such as phospholipid levels, is normal.288 335
8.2.4 Cementum
The apical cementum thickness triples or even quadruples (from about 150 µm) with age,350 406 including in impacted teeth.16 308 406 Human age is estimated using the cementum thickness in ancient and forensically recovered teeth,350 or by a microscopic count of the number of cementum layers deposited during life,355 which correlates highly with chronological age: Pearson’s r = 0.98 for persons up to 55 years. For older persons, a formula is used to adjust for discrepancies.351
Hypercementosis
Hypercementosis is a post-developmental, anomalous increase in the deposition of cementum, mainly at the apex, within the furcation and, in case of periodontal problems, at the proximal root surfaces.
The causes are either idiopathic,16 for instance in impacted teeth,161 363 or local and systemic, or drug-induced.281 Hypercementosis may delay eruption and is a secondary cause of root curvature and ankylosis.272
Local Causes
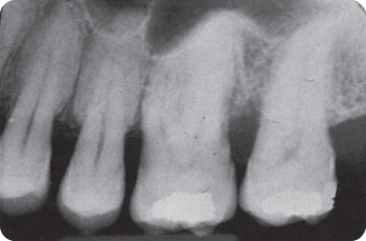
Almost 2% of 42-years-olds showed hypercementosis in an average of 3.8 teeth, mainly the second and first premolars and first molars, in this order.105 272 Others have found lower prevalence rates (0.1–0.3% of teeth).161 346 Excessive eruption after extraction of an antagonist, heavy occlusal forces and forced premature functioning of transplanted and partly developed teeth are associated with hypercementosis.231 232 346 363 391 Periodontal infection may lead to hypercementosis, either in the apical region or along the length of the root.183 217 363 Marked hypercementosis (Figure 8.3) makes a root club-shaped.76 The excess cementum may separate from the root during extraction.46 The periodontal space and the lamina dura of the bone are normal on radiographs (Figures 8.4 and 8.5).105 183
Figure 8.3 Club-shaped hypercementosis in a premolar and concrescence of two molars.

Figure 8.4 Hypercementosis in a first mandibular molar.
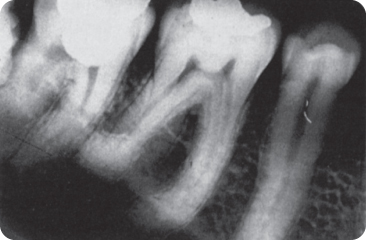
Figure 8.5 Premolars with hypercementosis, a feature also present in the other teeth in this dentition.
(Courtesy of N.A. Bakx.)
Acromegaly
Increased secretion of growth hormone factor by the hypothalamus (mostly due to an adenoma) leads to the release of excess growth hormone by the pituitary gland.100 The consequent increase in production of an insulin-like growth factor (IGF I) in the liver prompts skeletal growth, where the potential for growth is still present. In children there is gigantism, and in adults there is enlargement of, for instance, the terminal phalanges of the hands and feet. Swelling of the lips and submandibular glands may be the first sign.382 The face becomes coarse.369
Condylar growth leads to an increase in the size of the mandible, sometimes unilaterally.123 Lengthening of the mandibular body leads to the development of diastemata between the lower incisors and causes them to occlude anterior rather than lingual to the upper incisors (negative overjet). Pressure from the enlarged tongue contributes to development of an open bite.61 123 234 Hypercementosis has been observed in some adult patients in one or more teeth.105 391 Attempts to treat the open bite will be fruitless as long as the causative factor is not addressed.61
Osteitis Deformans (Paget’s Disease of Bone)
Osteitis deformans is a chronic bone disease in which: (1) an increased number of osteoclasts resorb bone at an increased rate; followed by (2) osteoblastic activity which leads to bone hypertrophy; and finally (3) sclerotic bone persists without an increase in turnover (rest stage).1 Viruses, e.g. the measles virus, have been demonstrated in the osteoclasts.56 255
Solitary lesions may remain unnoticed. In other cases, the accelerated resorption leads to soft bones that bend under weight-bearing. Later the bones become hard and their thickness increases. Secondary symptoms are caused by compression of the nerves by the hypertrophic bone (headache, deafness, blindness, facial paralysis). Sarcomas may develop.29 52 56
Hypertrophied facial bones give the patient the appearance of a lion, leontiasis ossea, which may be considered as a separate disease entity.67 In some 20% of patients, the jaws are involved, the maxilla twice as often as the mandible. Extraction may lead to jaw fracture,340 and in the osteolytic phase there may be prolonged bleeding, and in the osteo-sclerotic phase, a “dry socket” may result.52 330 Pressure from the widened alveolar ridge may lead to fracture of a prosthesis or a prosthesis may cause ulcers in the mucosa. The teeth in the enlarged and broadened alveolar processes become loose and spaced, and may exfoliate spontaneously.330 Later, sclerosis is observed around the tooth apices together with hypercementosis. The pulps are obliterated. Hypercementosis leads to ankylosis: the periodontal space and the lamina dura are absent on X-rays.46 189
The therapy is symptomatic: plicamycin administration prevents sarcoma and heart failure. Calcitonins are used to stabilise the calcium metabolism. Diphosphonates and sodium fluoride may prevent resorption.52 56 340 Use of gallium nitrate is still in experimental stages.1
Other Causes
Hypercementosis is associated with hypothyroidism, calcinosis (mineral deposits in soft tissues), arthritis, hypovitaminosis A and hypervitaminosis D, and some syndromes, such as the oculodentodigital syndrome, in which there is enamel hypoplasia and syndactyly as well as eye abnormalities with hypertelorism.38 55 81 109 In acute rheumatism, hypercementosis appears more radiolucent on X-rays than normal cementum.217 Autosomal dominant cementum dysplasia, an inherited anomaly, affects the cementum and adjacent bone. It is not clear whether the dysplasia, just like benign cementoblastoma,162 belongs to the group of hypercementoses.322
Ciclosporin A, an immunosuppressive agent that prevents rejection of transplanted organs, has been shown to induce the formation of large volumes of new cementum with an irregular outline, in particular in the cervical third of the roots.14
8.3 Nomenclature
Physiological attrition is tooth wear caused by particles in masticated food pulp, which exert a cutting action under the masticatory forces; the term is also applied to tooth wear caused by non-functional tooth contacts. Pathological attrition is tooth wear caused by chewing with a mutilated dentition and parafunctional movements (non-functional movements). Abrasion is tooth wear caused by frictional contact with foreign bodies other than food and tooth brushing. The occlusal, facial and lingual surfaces are affected.117 In particular circumstances, tooth wear progresses rapidly, and is distinguished by the cause.39 117 144 145 219 380
The term “attrition” did not become popular. Tooth wear due to tobacco chewing has been classified as abrasion,71 380 pathological attrition320 and attrition.329 In several countries, “abrasion” is used to refer to all kinds of tooth wear,271 317 and even to indicate erosion,260 and is also called corrosive wear205 and corrosion.117 Physiological attrition has also been called “abrasion”.407 Furthermore, other conditions have been distinguished:116 144 180 258 abfraction, which is the fracturing of cervical enamel and occlusal splintering of thin enamel under physical stress; and demastication, which refers to mesiodistal grooves in the incisal edges and cupping on occlusal surfaces caused by contact with hard food or foreign bodies.
Many clinical cases do not fit neatly into the categories mentioned above, and are often not readily diagnosed;17 this is also because several causes of tooth wear can act on a tooth simultaneously or at different points in time. The term “wear” covers all the categories mentioned above,260 although the different origins of tooth wear may be of preventive importance.
8.4 Physiological and Progressive Tooth Wear
Tooth wear is characterised by well-demarcated wear facets, which are related to the tooth contacts186 and there is a close fit between opposing facets.
Vigorous and prolonged mastication is a characteristic solely of mammals, and their teeth undergo wear. Compensatory mechanisms and adaptations (ongoing eruption, cementum deposition) guarantee an efficient masticatory system for the lifetime.241
The degree of wear differs greatly between the two dentitions. A balanced physiological state is said to exist when the distance between the occlusal plane and the alveolar crest remains constant throughout life,31 267 396 but when wear compromises functioning or survival of a tooth, the process is considered pathological.
Skeletal material excavated in Athens, near the Acropolis, is representative of almost the entire time span between the Neolithic period and the Turkish Domination, and of persons of all ages. The material showed that the occlusal plane-to-bone distance remains constant during life, in spite of tooth wear, except when the wear is pathological. In the physiological process, the length of the crown may be reduced to zero or even less than that, with root separation.267 A Romano-British population study supports the findings. Tooth wear is compensated by movement of the teeth in occlusal direction.396
In contemporary humans, a small amount of tooth wear underlies the increase in the lower face height (∼0.4 mm/year)397 because of alveolar bone growth and continuing tooth eruption. The cementum becomes exposed.241
Deciduous Dentition
Wear starts at the incisal edges of the incisors in an edge-to-edge bite (Figure 8.6). Next the occlusal molar surfaces are affected. Wear often progresses into the dentine (Figure 8.7).
Figure 8.6 A deciduous dentition showing incisal wear.

Figure 8.7 The wear has exposed the dentine of the deciduous teeth.

In contrast with deciduous molars, the spaced deciduous anterior teeth do not come into contact with each other and are not flattened approximally. The wear is in general most severe in the maxillary arch and the anterior teeth.387
Permanent Dentition
Occlusal wear in the permanent dentition starts in the teeth that erupt first, commonly the permanent mandibular first molars. Wear facets on cusp tips increase in size, rapidly or slowly, as the case dictates. The cusps become shorter and flatter.228 The masticated food leaves scratches on the enamel. Abrasive particles trapped in the scratches cause wear of the antagonists.205
Next, the incisor mamelons disappear, together with the height differences between the perikymata and imbrication lines. A normal bite is associated with labial wear facets on the incisal edges of the mandibular incisors and palatal facets on the maxillary incisors. A reversed bite causes wear on the opposite surfaces. The first mandibular incisor has one antagonist and thus shows one wear facet; the lateral incisor has two antagonists and two wear facets.
As more permanent teeth erupt, more tooth contacts are made, which slows down the tooth wear.334 The buccal cusps of the mandibular posterior teeth and the palatal cusps of the maxillary posterior teeth, called centric cusps or stops, receive the brunt of the forces during mastication. The deeper enamel that is thereby exposed shows normal ultrastructure.256
Over time, tissue loss may be substantial (Figure 8.8). Differences in incisal heights are gradually levelled and cusps in the post-canine zone become flatter. The wear progresses more rapidly when the dentine is exposed. The enamel of first molars already shows in teenagers (erosive) cupping (ditching) near the mesio-buccal cusp tip. Penetration of dietary agents discolours the exposed dentine brown.372 The incisal edges have a margin of white enamel surrounding brown discoloured secondary dentine; in the centre is the darker tertiary dentine. However, the core may be white.
Figure 8.8 Excessive wear of the permanent anterior teeth (possibly the result of parafunction).

Approximal wear occurs because the fibres of the periodontal ligament allows the teeth to rub to against each other during functioning, which together with the action of food flattens the approximal contact points. Mesial migration of the (pre)molars maintains the tooth contacts. The occluso-gingival width of the contacts increases from 1.5–2.5 mm to 3 mm. The bucco-lingual width of 2–3 mm broad contacts becomes 4–4.5 mm. Thereafter, wear reduces progressively because of greater resistance of the enlarged contacts.267
In the Lengua Indians (Paraguay) living in primitive conditions, approximal wear decreased after the eruption of the third molars.164
8.4.1 Measurements
The absence of stable reference points impedes quantitative measurement of occlusal wear. The upper border of the mandibular canal provides a fixed reference line that allows measuring the distance to the mandibular occlusal surfaces. There is no maxillary reference line.241
A number of qualitative indices are available to record occlusal wear, often using photographs or stone casts. Qualitative indices are non-linear and mean values are misleading. Broca’s index (1879) for occlusal wear372 was suggested to be arbitrary, ambiguous and subjective. The distinction between various tooth wear stages is relative:211
- 0 = no wear
- 1 = wear, but cusps still present
- 2 = occlusal dentine partly denuded
- 3 = only peripheral enamel present
- 4 = wear progression to or near the amelo-cementum junction.
Other scales, sometimes modified, are similar to Broca’s index.97 150 151 338 An eight-point scale, which was later modified,104 295 used quantitative and morphological criteria.227 Other indices assess the ratio between the denuded dentine and the total occlusal surface,228 385 the morphology of the centric and non-centric cusps,113 and the distance from the cusp tips to the intersection of the occlusal grooves (which, however, also undergo wear).229
The Tooth Wear Index (TWI) records per tooth the extent of (1) occlusal, lingual, buccal, (2) incisal and (3) cervical wear. Per age decade, “acceptable” threshold wear values have been proposed per tooth type,338 339 but age itself neither causes the defects nor determines the effects.42 83 Because of the difficulty in distinguishing wear from erosion, the index is applicable in both cases.
The Incisal wear Index (IwI) for children records the disappearance of the mamelons, followed by presence of smooth wear facets and finally incisal “ditching”.333 Ryge’s scoring system (Table 8.1) aids treatment decision making. A score is given corresponding to the most severe wear category of 90% of the tooth ratings. Colour photographs illustrate the wear stages.253
Table 8.1 Rating scale (simplified) for occlusal wear253
| Rating | Operational explanation |
| Satisfactory (= acceptable wear) | |
| R (Romeo) | Neither visible wear nor change in anatomical form |
| S (Sierra) | Limited (normal) wear. Limited change in morphology (enamel wear facets, small areas with exposed dentine) |
| M (Mike) | Considerable wear with obvious morphological change (length reduction, large dentine exposures without sensitivity) but without need for treatment |
| Non-acceptable wear | |
| T (Tango) | Considerable wear with marked morphological changes (tooth length reduction, large areas of exposed dentine that is soft and discoloured). Further damage to teeth and surrounding tissue is likely |
| V (Victor) | Excessive wear. Extreme morphological, aesthetic and functional changes (fracture of tooth tissues, soft dentine, pulp exposure, pain, gingival irritation). Damage to the teeth and/or surrounding tissues is now occurring |
8.4.2 Determinants of Wear
A number of partly interdependent factors determine the rate of tooth wear.
Age
Wear is age dependent,233 250 as in ancient humans,267 but cultural, regional (diet) and individual differences confound the determination of average tooth wear rates.177 229 274 332 Many children, teenagers and young adults show wear, and nearly 100% of older people, often into dentine.140 222 333 The almost equal tooth wear scores in younger and older people indicate that wear starts at an early age.326 Incisal wear is not related to loss of the posterior teeth. Unacceptable increase in wear (TWI) has been proposed as 5% for <15-year-olds and 9% for those >65-years-old.342 From the fifth decade onwards, wear in the canines and (pre)molars is not unrelated, probably because the canine guidance also disappears.325
In an Inuit study and in ancient Anglo-Saxon skulls, tooth wear was found to be an accurate predictor of age.227 241 Wear of contemporary 10-year-old bruxists predicts wear reasonably well 20 years later,169 but generally, age explains only 12% of the wear over the whole dentition.298 Sollberg et al. found that the correlation between age and premolar wear was 0.7 and with the anterior teeth 0.2, but correlations between wear and age vary considerably,345 due to scoring methods, differences in wear in different tooth, dietary differences (carbonated drinks),221 salivary composition and flow, participation in craft activities, etc. Scores in a sample of young Saudi Arabians varied depending on variables such as nail- and pen-biting, an erosive diet, use of a “miswak” (chewing stick used as a toothbrush) and bruxism. Tooth wear is more pronounced in Saudi Arabia than in Western countries, because of presence of fine airborne dust particles in the desert environment.150 151
Diet
Consumption of hard or uncooked foods promotes occlusal and approximal wear in both dentitions.135 143
The varying food of evolving hominids maintained the versatility of the omnivore.89 Davies et al. found that wear in Western Greenland was less than in the more isolated Eastern Greenland, where the food requires heavy and long mastication.72 Marked wear occurred in ancient tribes and populations due to consumption of uncooked food, methods of food preparation, and contamination of the food with sand.31 71 94 130 135 175 176 181 184 211 228 229 303 311 385 The hunter-gatherer community had more anterior tooth wear at a younger age than the later farming settlements due to habits; the molars in both groups were equally worn. At an older age, farmers lost their posterior teeth through caries, which promoted wear of the anterior teeth, contrary to the more contemporary findings noted above.143
Anthropologists use the degree of tooth wear as a benchmark for age determination. For example, an individual who died at age 13–14 years will show severely worn first permanent molars due to consumption of an abrasive diet but unabraded second premolars.31 Food availability and religious and cultural factors and habits largely determined the diet71 and underlie marked differences in tooth wear in prehistoric humans, which precludes age determination based on tooth wear alone. The diet must be studied, based on, for example, fossilised excrements.
A medieval population (AD400–800) exhibited more occlusal wear and cupping than an age-matched contemporary group with an acidic, raw diet, while the latter showed greater wear than their contemporaries with an average diet. Buccal concavities were common in the acidic diet group (63%), infrequent in the average diet group (8%), and absent in the medieval group.104
Masticatory Force/Time
Men tend to have more tooth wear than women91 151 326 342 345 because their masticatory muscles are more developed.70 152 329 386 Kiliaridis et al. found that subjects with advanced wear had a comparatively high biting force.165 Chewing times depend on the diet: a sample of 7000-year-old Indian dentitions showed considerable wear as a consequence of long and forceful mastication of raw vegetables and seeds.135
Saliva
Reduced saliva and salivary proteins, in particular lubricating mucins and proline-rich proteins, and a low buffering capacity, promote tooth wear.91 152 345 372 374 The permanent viscoelastic salivary film on tooth surfaces reduces friction.374 Ligation of the salivary gland ducts in rats increased tooth wear.54 Many medicaments, especially used by older persons, cause xerostomia (Chapter 5). Otherwise, salivary glands of elderly people function well, although mucin content decreases.381 It is not clear whether salivary lubrication is thereby substantially affected. Excessive tooth wear (enhanced by consumption of erosive beverages) has been reported in dehydration (leading to a reduced salivary flow) and in drug-induced xerostomia.405
Other Factors Causing Wear
Crossbites are associated with severe wear of the deciduous molars and a Class III canine relationship is associated with wear of incisors.387 Angle’s Class II and III molar relationships are associated with deviating wear patterns.326 The presence of some types of amelogenesis and dentinogenesis imperfecta increases the likelihood of tooth wear as fluoride may do.210 In diabetes mellitus, the first permanent molars develop typical saucer-like wear facets occlusally.283 Excessive wear in 100 patients was caused by “erosion” (in 35) and by “erosion-attrition” (in 25),329 as were the teeth in a pygmy.365 In a sample of young swimmers and cyclists using sport drinks, incisal edge tooth wear into dentine was found to be the rule than the exception.220 (Rough) porcelain and ceramics promote tooth wear, other restoratives hardly.
Contact with quartz-filled composite restorations in antagonist teeth affect/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


