Chapter 8
Permanent Dentition: Concussion, Subluxation, Lateral Luxation, and External Resorption
Aim
To provide a review of current practice for the treatment of tooth concussion, subluxation, lateral luxation and external resorption in the permanent dentition.
Outcome
After reading this chapter the reader should be aware of the appropriate treatment for concussion, subluxation, lateral luxation injuries and external resorptive lesions.
Aetiology
Luxation injuries are the least severe injuries to the periodontal ligament and immediate repositioning, and splinting will usually be successful in preventing permanent damage to the periodontal ligament. Flexible splinting techniques for two to three weeks are generally agreed to encourage physiological repair of the periodontal ligament and were discussed in the previous chapter.
Diagnosis
Accurate diagnosis allows correct treatment planning and increased likelihood of a successful outcome and it is worthwhile defining accurately the terms concussion, subluxation and lateral luxation:
Concussion: This results from a jarring impact on the tooth and there may be both oedema and haemorrhage within the periodontal ligament, causing the tooth to be tender on biting. However, the tooth is not mobile and no evidence of periodontal ligament bleeding is visible.
Subluxation: The impact is greater and results in a loosening of the tooth in the socket and visible periodontal ligament haemorrhage and tenderness on biting. The tooth, however, is not displaced and is still within the line of the arch.
Lateral luxation: The horizontal impact displaces the tooth from the line of the arch in either a labial or palatal direction (Figs 8-1a, b and 8-2). Mesial or distal luxation can occur, but is not as common. The displacement of the tooth invariably involves a fracture of the alveolar socket walls and more damage to the periodontal ligament and obvious haemorrhage. The occlusion may be significantly affected by the displacement. A parent’s knowledge or indeed an old photograph can be helpful if any doubt exists about the position of a tooth and whether its position has changed.
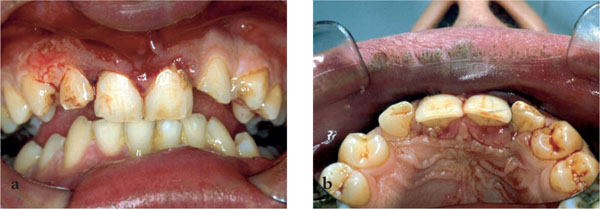
Fig 8-1a,b Palatally luxated 11,21.
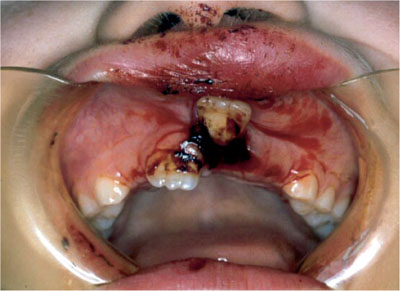
Fig 8-2 Labially luxated 21.
In all of these injuries there may be pain on slight digital pressure on the tooth. Percussion tests are not advisable. The amount of damage to the neurovascular bundle will depend on the degree of displacement. Radiographs must be taken of each traumatised tooth:
-
Periapicals are usually the most appropriate. If there is a lot of sensitivity from an injured tooth then an anterior occlusal may be a better option.
-
All teeth suspected of sustaining an injury should be included.
-
Separate views at different angulations may be required to detect a root fracture.
Treatment
Concussion and Subluxation
Although concussion and subluxation are the mildest of periodontal ligament injuries, it is still vitally important to protect the neurovascular bundle from further damage. The treatment for both these injuries, especially if the affected tooth has a closed apex, is:
-
occlusal relief
-
soft diet for seven days
-
immobilisation with a splint
-
chlorhexidine 0.2% mouthwash, twice daily for plaque control.
Pulpal Necrosis and Root Resorption
Data for pulpal survival after these injuries indicate that there is minimal risk of pulpal necrosis in the tooth with an open apex, but 15% of those with closed apices become non-vital. These data endorse the importance of immobilisation and splinting, especially in the closed apex tooth, to protect the neurovascular bundle. The incidence of any form of resorption is very low.
Lateral Luxation
There is damage to periodontal ligament, pulp and the alveolar plates, and treatment is more extensive:
-
Local anaesthetic (labial and palatal) is required if there is an alveolar plate injury.
-
Atraumatic repositioning with gentle but firm digital pressure.
/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


