8
Molar Protraction
Conventional anchorage provides very limited options for anterior anchorage reinforcement during molar protraction, especially in the mandibular arch. It typically involves using the anterior teeth as the anchorage unit, but this is limited by these teeth’s relatively low combined root surface areas. Consequently, many orthodontists are historically reticent to attempt closure of large posterior spaces, especially if alveolar necking is present. Fortunately, mini-implant anchorage now means that many more such patients can be treated orthodontically, although one still needs to be realistic in terms of the difficulties posed by alveolar deficiencies. Therefore it is crucial to assess the feasibility of space closure in terms of both the anchorage requirements and the edentulous site anatomy. In lieu of surgical alveolar ridge augmentation, substantial reductions in alveolar height and width may severely limit mesial movement of the posterior teeth, especially in hypodontia cases (where the alveolus is hypoplastic) or long-standing edentulous sites (where it has atrophied). Furthermore, the molar which is adjacent to the distal aspect of such an alveolar problem is much more prone to mesial tipping problems, although there are now biomechanical solutions for this problem whereby bodily movement can be promoted.
Mini-implant sites in the mandibular arch are limited to the buccal aspect of the alveolus, whilst maxillary protraction can utilise options of either buccal and palatal alveolar (direct) or mid-palate (indirect) anchorage.
Clinical objective
- To prevent distal movement of the anterior teeth during molar protraction for closure of a posterior space (e.g. a second deciduous molar or permanent molar site).
Treatment options
- Buccal alveolar mini-implant anchorage (direct or indirect) in either arch.
- Palatal alveolar mini-implant (direct) anchorage.
- Indirect anchorage of upper incisors using mid-palate mini-implant(s).
- Mid-palate mini-implant protraction appliance (reverse distaliser).
- Indirect anchorage using buccal mini-implants for intermaxillary traction.
- Conventional anchorage, e.g. protraction headgear or intermaxillary elastics.
- Alteration of the skeletal base by orthognathic surgical or orthopaedic appliance treatments, in order to offset anterior anchorage loss (incisor retraction).
Key treatment planning considerations
- The molar, incisor and centreline relationships.
- The quantity and quality of the alveolar ridge in the edentulous space. If a tooth is still present here, then is it ankylosed, or did infection or other pathology cause bone loss?
- The depth and shape of the palatal vault, since a high arched palate makes it difficult to insert mini-implants in the mid-palate.
- The interproximal bone volume at the proposed mini-implant (alveolar) site, in terms of both the mesio-distal space (root divergence) and bucco-lingual alveolar depth. Limitations in both dimensions mean that an oblique angle of mini-implant insertion and possibly a shorter body length are preferable. Alternatively, as suggested by experts such as German orthodontist Dr. Björn Ludwig, a long mini-implant may be inserted perpendicular to the surface with the aim of bicortical engagement. This option requires additional lingual anaesthesia and then composite resin coverage of the mini-implant tip, if it projects beyond the lingual tissues, risking tongue irritation. In addition to the benefit of bicortical anchorage support,1 this lingual projection may also be used to provide supplementary traction to the lingual side of the molar, hence reducing the risk of molar rotation during mesialisation.
- The amount of mesialisation required and whether this differs on each side of the arch.
Biomechanical principles
- Hypodontia cases may have limited alveolar bone width/height at the mini-implant insertion site. This especially affects insertions adjacent to the canine eminence, which may be under-developed if the canine erupted in an ectopic position.
- Prepare the fixed appliance ready for mini-implant insertion (by divergence of adjacent roots) and the simultaneous initiation of space closure by progressing to a rigid working archwire, e.g. a 0.019 × 0.025 stainless steel one.
- If a lengthy period of initial alignment is required, then consider delaying any extractions, especially of ankylosed deciduous molars, until the arch is ready for the immediate start of space closure. Otherwise, alveolar resorption may occur at an already compromised site and limit space closure.
- Forces applied at the coronal level will tip molars mesially during protraction, especially if there is a vertical alveolar deficiency on the mesial aspect of the molar. This also tends to be worse if a second molar is not available or attached to help control the first molar alignment.
- Mesial tipping of molar teeth causes archwire binding and consequently frictional problems (Fig. 8.1), then possibly protraction (mesial shunting) of the entire dental arch and incisor intrusion. This manifests as a reduction in overjet and overbite (Fig. 8.2).
- The use of a posterior powerarm, to apply traction at the molar furcation level, assists bodily molar movement and unidirectional space closure. Powerarms may be free-sliding on the archwire (Fig. 8.3) although they provide better bodily control when attached directly to a molar crown. The latter approach involves placement of a double tube attachment on at least one molar per dental quadrant, then fabrication of a steel powerarm from a piece of rigid archwire, e.g. 0.021 × 0.025 size (Figs 8.4 and 8.5).
Figure 8.1 Diagram of the side-effects of oblique traction from an anterior mini-implant to the first molar hook and a reduction in the adjacent alveolar height: molar tipping causes archwire binding and advancement, resulting in incisor protraction and intrusion.
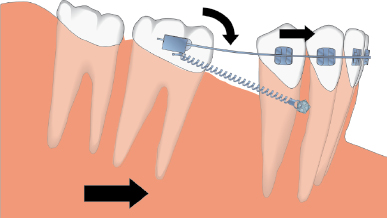
Figure 8.2 An adolescent girl with a Class II division 1 malocclusion and absent second premolars. (a) An oblique vector of elastomeric traction was applied from the mandibular mini-implant, inserted mesial to the first premolar, directly to the first molar hook. This resulted in (b) a reduction in the overjet and overbite as the lower incisors proclined and intruded. Elastomeric traction was then added between the molar and archwire hooks, to prevent mesial movement of the archwire. (c) Control of the incisor relationship had been achieved after eight weeks of combined traction and (d) continued during the complete phase of molar protraction.

Figure 8.3 An adult Class III patient who required protraction of the lower right second and third molars prior to a mandibular osteotomy. Chronic infection had resulted in severe alveolar bone loss in the first molar area. (a, b) Two mini-implants were inserted, because of the anticipated difficulties with space closure, and elastomeric traction connected to a sliding powerarm (on the archwire distal to the second molar tube) and third molar hook. (c, d) Space closure was achieved with bodily molar mesialisation.

Figure 8.4 Diagram of bodily molar protraction utilising a powerarm connected to the molar tube to achieve a horizontal vector of traction.
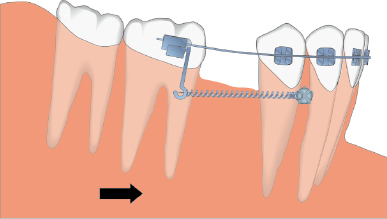
Figure 8.5 An adult patient with a double molar tube bonded on the upper left second molar. A 0.019 × 0.025 steel wire has been used to fabricate a powerarm which engages the auxiliary molar tube and mirrors the vertical level of the mini-implant.

Mid-treatment problems and solutions
- Ideally only apply traction to a powerarm in order to optimise bodily molar movement.
- Bond or band the second molar, in each relevant quadrant, since this helps to control mesial tipping of the first molar and enables direct closure of any inter-molar spaces.
- A shallow posterior buccal sulcus depth may prevent initial placement of a powerarm, especially on the terminal molar, but this can be added once sufficient mesial movement of the molar moves it into an area with more sulcus depth.
- If there are signs of unfavourable incisor intrusion then add a bite-closing curve to the archwire.
- If incisor advancement and proclination occur, as a result of archwire binding, then consider adding supplementary traction from the molars to the anterior teeth or archwire hooks (Figs 8.2b, c).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


