Clinical and surgical techniques
Simrit Malhi, Angus C Cameron and Rebecca Eggers

Extraction of teeth in children
The removal of teeth in children can be one of the most stressful procedures for both the operator and patient. While a tooth may be totally anaesthetized, the pressure felt during the extraction can be extremely upsetting and uncomfortable. As one of the most important aspects of clinical practice, dentists need to be skilled, efficient and sensitive in the removal of teeth in children. Teeth should be removed gently with good surgical technique rather than excessive force that may fracture roots or upset the patient.
General principles of tooth extraction in children
Preoperative assessment
Other principles

Anterior teeth




Premolars
Molars
• Extractions should be clean and atraumatic.
• Avoid gingival injuries by freeing the gingival margin with a flat plastic, luxator or elevator (Figure 8.3).


• Support the alveolus on either side with fingers.
• ‘Cow-horn’ pattern forceps are extremely useful in removing either upper or lower permanent molars, especially those with little or no crown remaining on the lingual aspect (Figure 8.5).







Avoiding and managing root fractures
Following the extraction
Postoperative instructions following extractions for children
Always give clear and lucid instructions to the child and caregiver:
Repair and suturing of soft tissue injuries
Generally, soft tissue wounds should be closed within 24 h. Good closure of wounds allows for more rapid healing by primary intention. Suturing may reduce the sequestration of displaced bony fragments and may prevent bacterial contamination of the gingival sulcus. Furthermore, there is much less pain from the wound if exposed bony defects are well covered with periosteum and gingival tissues. Deeper lacerations of the lip will involve the muscle layer and it is important to close this as a separate layer to prevent formation of a ‘dead space’ will easily become infected (Figure 8.6). It is essential that the wound is properly debrided and free of contamination from foreign bodies or bony spicules prior to apposition of tissues. Any wound involving skin, including those crossing the vermillion border of the lip, require precise and expert skill to facilitate the best possible result. Often, this requires timely referral to an appropriate surgeon.


Cyanoacrylate (tissue glue) is now commonly used for closure of smaller soft tissue wounds on the face and scalp in children without having to give local anaesthetic. Currently, the literature is equivocal as to whether suturing or gluing produces better outcomes, although it is clear that gluing is far less traumatic for the child and much faster.
Choice of material (Table 8.1)
The choice of suture material and needle will depend on:
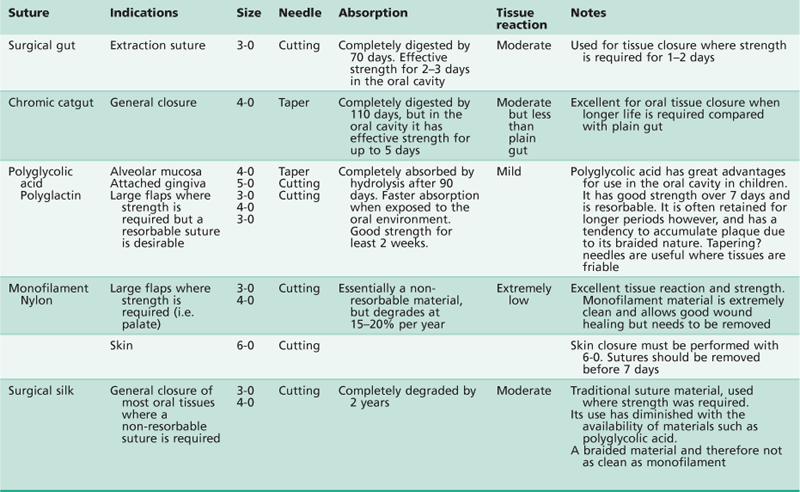
The type and location of the wound to be closed

The required strength and length of time required
Whether the material needs to be removed – resorbable or non-resorbable
Instruments
While each surgeon will have their own individual preference of surgical instrumentation, the following instruments are those commonly used in many oral surgical suturing situations.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


