7
Management of Anterior Crossbites
Prevalence of Anterior Crossbite Malocclusions
The U.S. Public Health Service surveyed the incidence of anterior crossbites in a large sample of whites, blacks, and Mexican Americans from 1988 to 1991 (Brunelle, Bhat, and Lipton 1996). The subjects examined ranged from 8 to 50 years old. Subjects with zero overjet totaled 4.4% of the sample. Subjects having from −1 to −4 mm of anterior crossbite totaled 0.8% of the sample. The percentage of potential patients who need treatment for this malocclusion problem is about 5% (Table 7.1).
Table 7.1. Distribution of Overjet among Americans Ages 8 to 50 Years, 1988–1991*
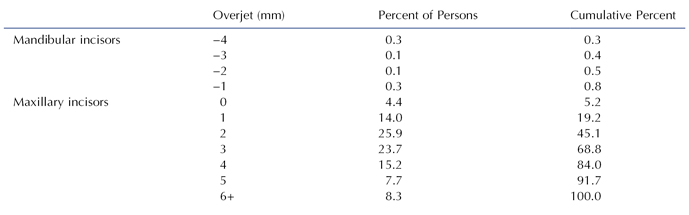
*From Brunelle, Bhat, and Lipton (1996).
Angle Classification
Observe the Angle Classification of the molars and canines. The best candidates for minor orthodontic treatment are those with a Class I molar and canine occlusion or a super Class I occlusion in centric occlusion in association with a forward anteroposterior shift from centric relation to centric occlusion.
Centric Relation to Centric Occlusion Functional Shift on Closure
Examine the patient who has an anterior crossbite for any evidence of a forward anteroposterior shift during closure of the mandible. Ask the patient if he can touch the incisal edges of his upper and lower incisor teeth together, in order to determine whether a forward shift is taking place. If the patient’s mandible shifts forward during closure from centric relation to centric occlusion, correction of the anterior crossbite will result in a posterior displacement of the mandible. If the patient with a forward shift has Class I molars in centric occlusion, correction of the anterior crossbite will eliminate the forward shift and tend to make the molar occlusion end-to-end. If the patient with a forward shift has a Class II molar relationship in centric occlusion, treatment of the crossbite will eliminate the shift and tend to make the molar occlusion more severely Class II. If the patient with a forward shift has a Class III molar relationship in centric occlusion, treatment of the crossbite will eliminate the forward shift and tend to make the molar relation less severely Class III. For patients who have an anterior crossbite associated with a forward anteroposterior shift, a slightly super Class I molar occlusion in centric occlusion before treatment is most desirable, because correction of the anterior crossbite would eliminate the shift and tend to alter the molar occlusion to Class I.
If no forward anteroposterior shift is present, the molar relationship will not change as a result of the crossbite treatment, making the diagnosis and treatment more straightforward.
Overbite
Moderate to deep overbite of the incisors is a favorable condition for successful treatment of an anterior crossbite, because the deeper overlap of the incisors will help retain the incisors brought out of crossbite. A removable appliance with a posterior acrylic bite block is needed in deep overbite patients to allow an appliance to move the upper incisors forward out of crossbite. Normal to deep overbite patients can be treated with both removable and fixed appliances. Because removable appliances have less control of the teeth than fixed appliances, removable appliances are best suited for patients whose teeth need to move short distances and are not rotated.
When a patient has little overbite or an anterior openbite, correction of the crossbite will require extrusion of the upper and perhaps lower incisors after the crossbite is corrected, in order to establish normal overbite. Without any overbite at the end of treatment, the upper incisor(s) can easily relapse into a crossbite. A maxillary Hawley retainer is needed to keep the tooth from relapsing back into crossbite. As an upper incisor is tipped forward with either a removable or a edgewise fixed appliance, its change in labial-lingual inclination tends to move the incisal edge upward (vertically), which in turn opens the bite. The finger spring of a removable appliance will often intrude the upper incisor as it pushes the crown forward, an action that also opens the bite. For these reasons, an edgewise fixed appliance is the best appliance for treating patients who have minimal overbite or frank anterior openbite. An edgewise appliance can move an incisor forward and also extrude it as needed to create overbite. Even then, the retention of the crossbite is a long-term concern. Patients with a frank anterior openbite should be referred to a specialist.
Adequate Arch Length
A tooth in crossbite cannot be moved out of crossbite, if the existing space in the arch cannot accommodate the tooth. If arch length is insufficient, the first priority in treatment is to create sufficient arch length. In minimal arch length deficiencies, shaving off a little enamel from the tooth itself and its surrounding teeth may be adequate. No more than 0.2 or 0.3 mm should be removed from a permanent tooth. Larger amounts of interproximal enamel can be removed from primary teeth that will eventually exfoliate. If spaces exist between other anterior teeth, these spaces should be closed to create adequate arch length and accommodate the tooth in crossbite. As arch length deficiency increases, it is more likely that a fixed orthodontic appliance will be needed to accomplish the treatment.
Spaces can be opened between teeth with finger springs mounted in a Hawley appliance and with compressed coil springs in the edgewise fixed appliance.
Inclination of Maxillary Incisor Roots
If the tooth in crossbite is positioned lingual to the line of arch (the line along the crest of an alveolar ridge that represents where the anatomic contact points of the teeth should be located ideally on that alveolar ridge) in the anterior palate, it will have to move a long distance to get it out of crossbite. The resulting increase of the labial-lingual inclination of the tooth will create a functional and aesthetic problem and increase the probability that the tooth will relapse back into crossbite. In order to correct the increased inclination problem, an edgewise fixed orthodontic appliance with a large rectangular arch wire must be used to torque the tooth and move its root labially into normal inclination. The farther a tooth in crossbite is positioned away from the line of arch, the more likely it is that the labial-lingual inclination of the tooth must be corrected with an edgewise fixed orthodontic appliance. The most appropriate teeth for minor treatment with a removable appliance are located a short distance from the line of arch.
Teeth most easily moved out of crossbite are those that are inclined lingually toward the palate. The orthodontic movement of these teeth during the correction of the crossbite should bring them into more normal inclination. Teeth that are inclined lingually are the best teeth to treat with a removable appliance.
Rotation of Tooth in Crossbite
If the tooth in crossbite is rotated on its long axis, a fixed orthodontic appliance is the most appropriate choice for treatment of the crossbite. Removable appliances cannot easily rotate teeth. A rotated tooth has a high potential for relapse following its treatment. When possible, a fixed retainer is bonded to the lingual surface of the rotated tooth and its surrounding teeth at the end of treatment in order to prevent the relapse of the rotation. When both central incisors are rotated prior to treatment, it is best to bond a fixed retainer to the lingual surfaces of both teeth to prevent relapse of the rotation after treatment.
Number of Teeth in Crossbite
The difficulty of the treatment increases with the increase in number of teeth in crossbite. When several anterior teeth are in crossbite, an edgewise fixed appliance provides the best treatment.
Alignment of Lower Anterior Teeth
Alignment of the lower anterior teeth, if needed, should be done after the crossbite problem has been corrected. Alignment of lower teeth before the crossbite is corrected will complicate the correction of the crossbite by increasing the distance required to move the upper teeth forward, and will delay the elimination of a functional shift, should one be present.
Treatment of Anterior Crossbites with Removable Appliances
A removable inclined plane (Bruckl appliance) can be used to correct anterior crossbites and retain the corrected occlusion (Jirgensone, Liepa, and Abeltins 2008).
A Hawley appliance can be used to correct an anterior crossbite (Hawley 1919). Several types of finger springs are shown in Figure 7.1. The double helical spring has a long range of action with reduced force (Fig. 7.1A). The question mark spring has a short range of action and a strong force (Fig. 7.1B). The Z or S spring has a long range of action and strong force (Fig. 7.1C). The eyelet arm spring is similar to the question mark spring (Fig. 7.1D). The mushroom spring is a combination of two question mark springs and has a short range and strong force (Fig. 7.1E). The mushroom spring is often used to move posterior teeth buccally. All the finger springs are fabricated from 18-mil (0.018 inch) stainless steel; have a leg of wire, which is embedded in the acrylic body of the appliance; and are activated by extending the spring toward the incisor in crossbite. The springs are bent in the laboratory to adapt passively against the lingual surface of an incisor with the free end of the spring usually on the mesial side of the lingual surface. From this initial position, adjustments to activate the spring must keep the wire well adapted to the lingual surface of the incisor. To keep the spring against the lingual surface of the incisor, it is usually bent toward the cingulum as well as advanced forward. The force on the cingulum tends to intrude the incisor. The force needed to tip a tooth with a finger spring ranges from 30 to 50 grams (Crabb and Wilson 1972). Small adjustments to activate the finger springs will produce forces in this range.
Figure 7.1. Finger springs used in the correction of anterior crossbites: (A) double helix or recurved finger spring, (B) question mark finger spring, (C) Z or S finger spring, (D) eyelet arm finger spring, and (E) mu/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


