CHAPTER 7
Immediate Implant-Supported Restoration of the Edentulous Arch
Stephen G. Alfano and Robert M. Laughlin
Department of Oral and Maxillofacial Surgery, Naval Medical Center San Diego, California, USA
A method of transitioning a patient with complete edentulism or a nonrestorable dentition to an implant-supported fixed restoration without the use of an interim removable prosthesis.
Indications
- Adequate bone volume for the placement of dental implants
- Adequate interarch distance for a fixed prosthesis
- Properly motivated patient to maintain a fixed prosthesis
Contraindications
- Uncontrolled systemic disease
- Retrognathic jaw relationship
Technique (Surgical)
- The procedure may be undertaken using local, intravenous, or general anesthesia.
- Extraction of the remaining dentition is carefully completed, making sure to preserve alveolar bone.
- The alveolar bone is curetted to debride granulation tissue, periapical pathology, and fistulous tracts.
-
The residual edentulous maxillary arch is leveled and reduced to ensure the interface between the abutment, and the final restoration is superior to the lip line during animation (see Figure 7.2 [all figures are in Case Report 7.1]).
-
The residual edentulous mandibular arch is leveled to achieve a uniform flat surface topography to provide the proper width for the placement of dental implants and sufficient vertical space to allow for restorative materials (Figures 7.5 and 7.6).
- Posterior implants are placed to ensure proper distal angulation to avoid violating vital structures (mental nerve, and maxillary sinuses) (Figures 7.3 and 7.5). Anterior implants are placed along the long axis of the anterior alveolus (Figure 7.6).
- Alveolar bone interfering with the seating of the abutments is removed.
- Abutments are seated and torqued to manufacturer recommendations.
- Healing caps are placed on the abutments, and the incisions are closed in a tension-free manner with resorbable sutures (Figures 7.4 and 7.7).
- Postsurgical films are taken to ensure appropriate implant position and complete seating of abutments.

Figure 7.1. Pretreatment panoramic radiograph; note existing anterior maxillary dental implants.
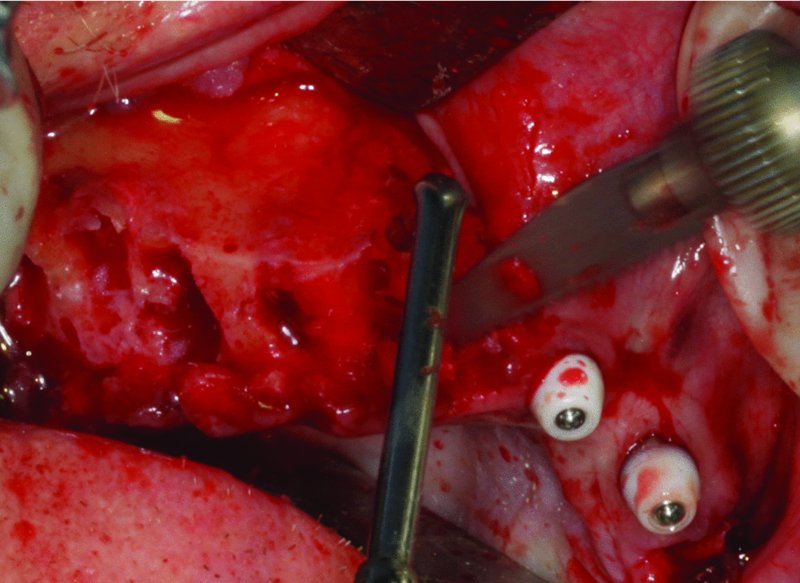
Figure 7.2. After extraction, the maxillary alveolus is leveled with a reciprocating saw.
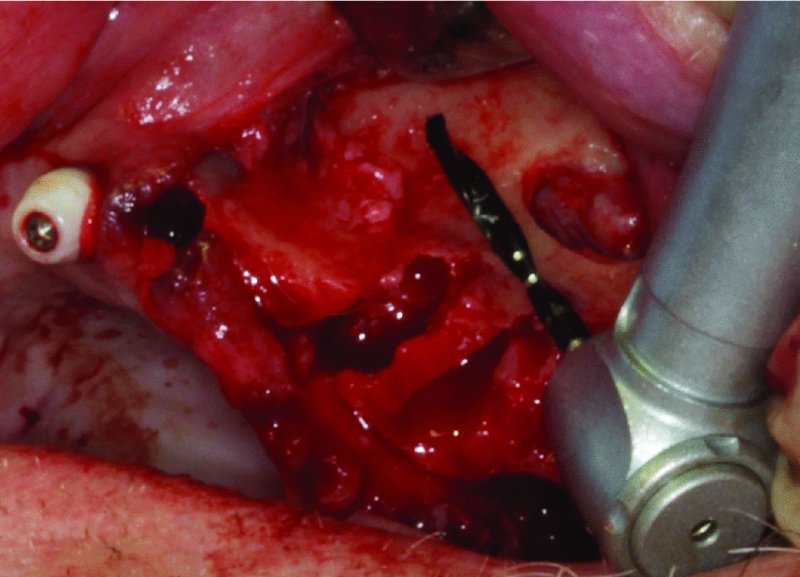
Figure 7.3. The sinus is located. The drill demonstrates the proposed angle of the distal implant to engage the medial sinus wall.
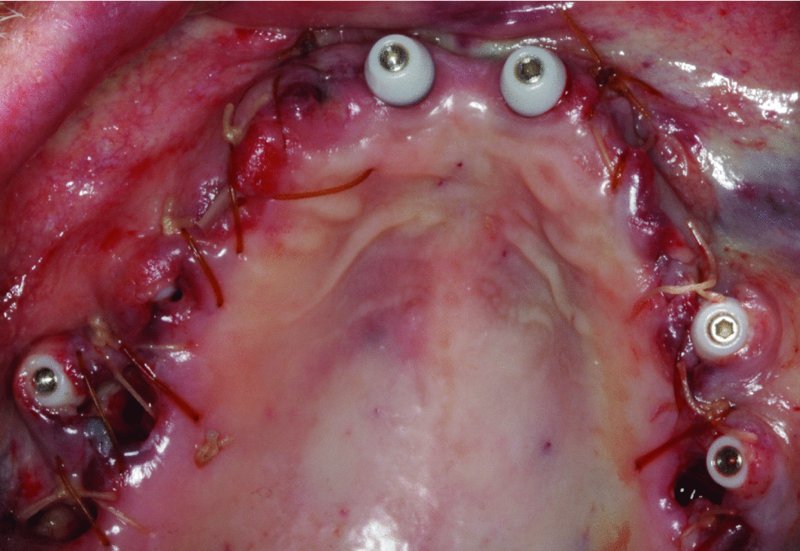
Figure 7.4. Maxilla immediately post-surgery and prior to the restorative process.
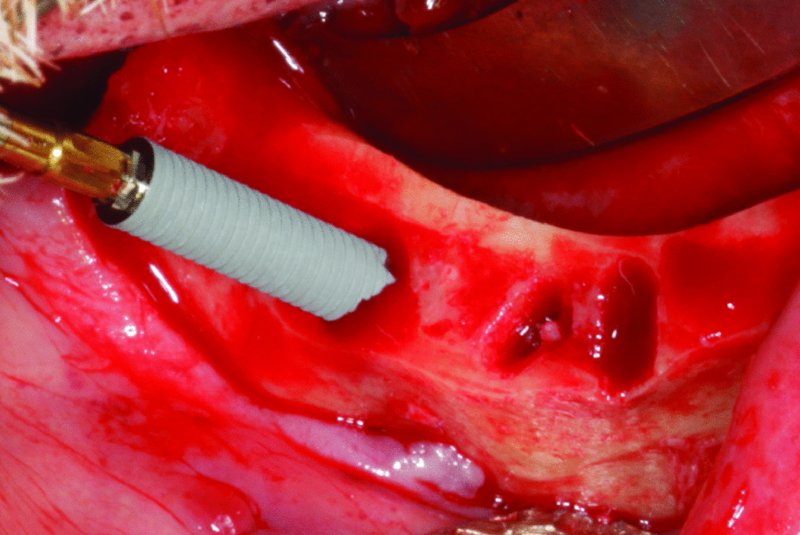
Figure 7.5. Mandibular arch after extraction of teeth and the creation of a flat broad table for implant placement. The mental nerve is identified, and the posterior implant is angled distally to avoid contact with the mental nerve and to maximize the anterior-posterior (A-P) spread of implants.
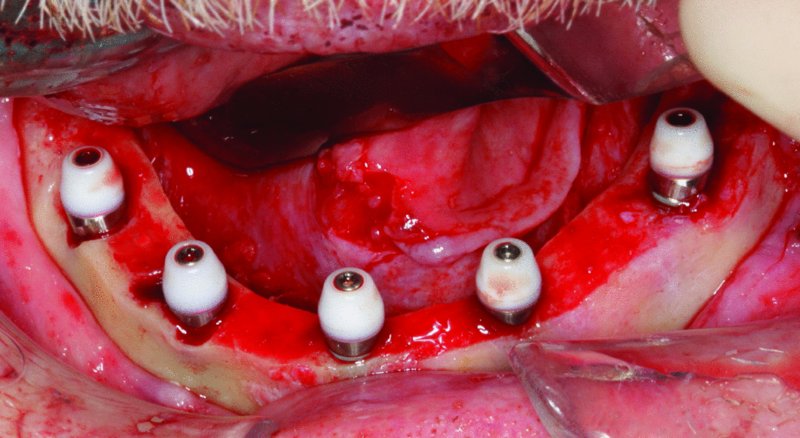
Figure 7.6. Mandibular arch post implant placement demonstrating the abutment locations and the anterior-posterior (A-P) spread. Both distal implants are angulated to increase the A-P spread.
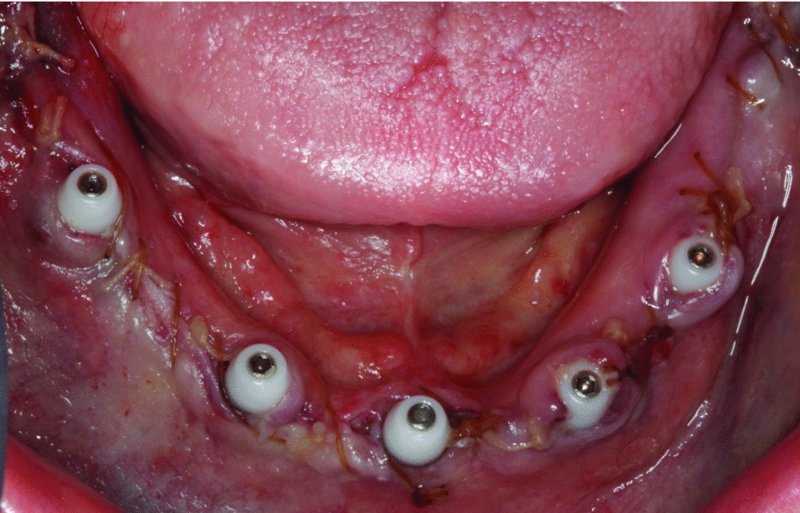
Figure 7.7. Mandible immediately post-surgery and prior to the restorative procedure.
Note: These procedures are typically performed in/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


