CHAPTER 30
Arthrocentesis of the Temporomandibular Joint
Robert M. Laughlin and James MacDowell
Department of Oral and Maxillofacial Surgery, Naval Medical Center San Diego, San Diego, California, USA
Procedure: Arthrocentesis of the Temporomandibular Joint
A highly successful minimally invasive procedure for the initial treatment of temporomandibular joint (TMJ) pain and dysfunction refractory to medical management.
Indications
- Medically refractory pain to TMJ muscles, headache, or earache impacting the patient’s quality of life
- Altered jaw mechanics such as closed lock, joint hypomobility, and limited range of motion in maximal incisal opening, excursion, and/or protrusion
- Alterations of occlusion
- Joint noises associated with pain
Contraindications
- Presence of concomitant facial pain of separate etiologies
- Chronic pain disorders
- Presence of deformity or pathology of the TMJ
- Presence of local or systemic conditions that may interfere with normal healing process and subsequent tissue homeostasis
Anatomy
- Temporomandibular Joint (TMJ): A compound synovial ginglymoarthrodial joint with rotation of the condyle within the inferior joint space. The TMJ has an overlying highly vascular and innervated fibroelastic capsule, which is thickened on the lateral aspect to form the temporomandibular ligament. The vascular supply to the TMJ is supplied with branches from the superficial temporal and maxillary arteries with an extensive venous plexus within the bilaminar zone.
- Articular eminence: A prominent convexity lined with dense, compact connective tissue that is subject to loading during function.
- Glenoid fossa: A nonloading, concave structure lined with a thin layer of fibrocartilage separated from the middle cranial fossa by 1–2 mm thickness of temporal bone.
- Articular disc: A biconcave avascular fibrocartilage disc that divides the joint space into a 1.2 mL upper compartment and a 0.9 mL lower compartment and allows complex movements of rotation and translation.
- Auriculotemporal nerve: Provides sensation to the posterior and lateral capsule.
- Masseteric nerve: Provides sensation to the anteriomedial aspect of the joint.
- Deep temporal nerve: Provides anterolateral sensation to the joint.
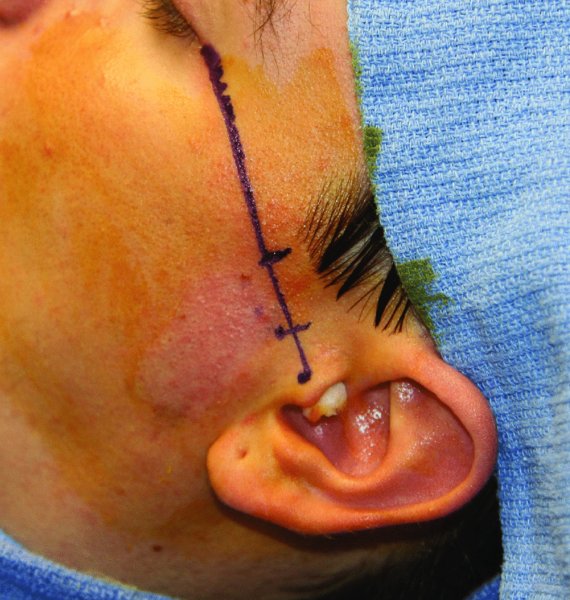
- Holmlund–Hellsing line (H-H line): A line extending from the lateral canthus of the eye to a point bisecting the tragus of the ear (Figure 30.1 [all figures cited appear in Case Report 30.1]). The 10-2 point (10 mm anterior and 2 mm inferior to the mid-tragus along the line) correlates with the posterior recess/glenoid fossa. The 20-10 point (20 mm anterior to the mid-tragus point along the line and 10 mm below the line) correlates with the prominence of the articular eminence.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


