6
Test Yourself
In this chapter, clinical cases will be shown and readers will be asked to decide whether use of an upper removable appliance (URA) is sensible or not and, if it is, to design an appropriate appliance. At the end of the chapter, the answers will be given and line drawings provided of a possible appliance design where appropriate. In some cases, more than one design may be feasible. If URA treatment is not appropriate, the reasons will be explained.
- When the use of a URA may be appropriate
- When the use of a URA may be inappropriate
- How appliances should be drawn and written on a laboratory card
Note that in these cases, it is assumed that any suggested treatment could only be undertaken once a full clinical examination had taken place and all necessary records had been examined by the operator. This would, of course, also include the necessary and appropriate radiographic and study model examination. The following cases are therefore intended only to give examples of what might be possible and where treatment should be avoided and/or a specialist opinion sought.
Note also that in all the mixed dentition cases that follow, and where the upper permanent canines are unerupted, that they are palpable buccally.
Questions
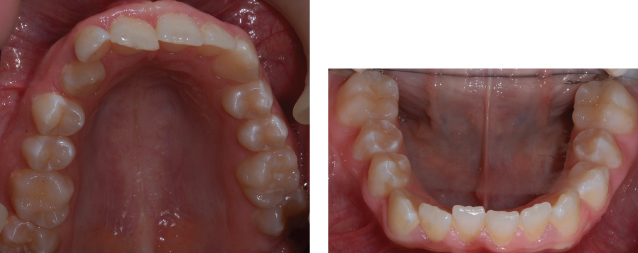
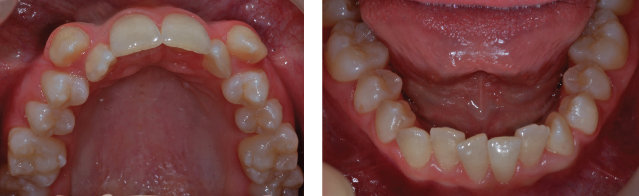
Case 1 (Figure 6.1)



This patient is 11 years old and has no complaints, but her mother is concerned about the crossbite of UR1. She has also noticed that LR1 is being displaced labially. There is a forward displacement on closure associated with the incisor crossbite and the patient is fit and well.
Carry out an orthodontic assessment of the patient and then answer the following question:
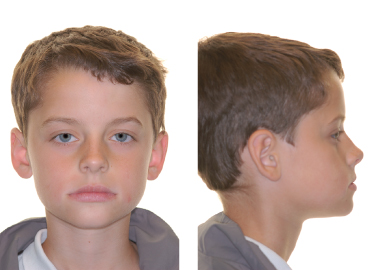
Case 2 (Figure 6.2)



This male patient is 11 years old and is concerned that his front teeth stick out. He has not had orthodontic treatment before. He is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following questions:
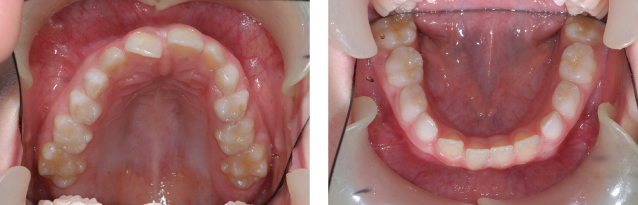
Case 3 (Figure 6.3)



This 12-year-old boy is concerned regarding his bite. He has a mandibular displacement anteriorly from an edge-to-edge incisor relationship. He is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following questions:
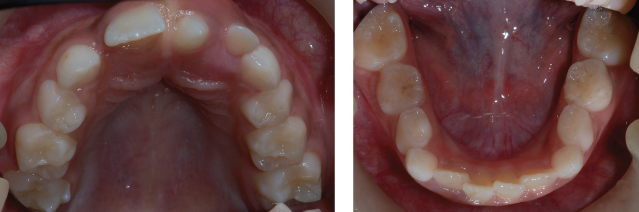
Case 4 (Figure 6.4)


This patient complains of crooked teeth. She is 13 years old and is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 5 (Figure 6.5)



This patient is 9 years old and has no complaints, but her mother is concerned about the crossbite of UR2. There is a displacement on closure associated with the incisor crossbite. The patient is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 6 (Figure 6.6)



This 24-year-old female patient is concerned about the appearance of her front teeth. She has had some orthodontic intervention before, which involved the extraction of UR4, LL4 and LR4, but no appliance treatment. She is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following questions:
Case 7 (Figure 6.7)



This 8-year-old patient was referred by his dentist regarding the posterior crossbite. The patient himself has no concerns and is fit and well. He has a mandibular displacement to the left of more than 2 mm off ULC.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 8 (Figure 6.8)

This patient is 8 years old and has no complaint, but his parents are concerned by his crooked teeth biting the wrong way round. There is a displacement on closure associated with the incisor crossbite. The patient is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 9 (Figure 6.9)



This 9-year-old patient has previously had a supernumerary tooth removed which was preventing the eruption of UR1. UR1 has not erupted any further for the past 6 months. The patient is concerned regarding the appearance of UR1. She is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 10 (Figure 6.10)


This patient is 8 years old and does not like the appearance of her top front teeth. The patient is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 11 (Figure 6.11)


This patient complains of crooked teeth. She is 13 years old and is fit and well. There is no displacement on closure.
Carry out an orthodontic assessment of this patient and then answer the following questions:
Case 12 (Figure 6.12)



This 8-year-old girl was referred by her dentist because UR1 has not erupted, although it is palpable high in the labial sulcus. She is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following questions:
Case 13 (Figure 6.13)



This patient is 11 years old and is concerned about his bite. He has had some orthodontic treatment with a URA before. He does not have a mandibular displacement and he is aware that oral hygiene needs to improve significantly prior to any orthodontic treatment being provided.
Carry out an orthodontic assessment of this patient and then answer the following questions:
Case 14 (Figure 6.14)



This patient is 8 years old and complains that you cannot see his top front tooth. There is a displacement on closure associated with the incisor crossbite. He is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 15 (Figure 6.15)



This 12-year-old female patient is concerned about the prominence of her upper front teeth. She is fit and well.
Carry out an orthodontic assessment of this patient and then answer the following question:
Case 16 (Figure 6.16)



This 11-year-old girl is concerned regarding the position of her front teeth. She is fit and well and has a mandibular displacement from an edge-to-edge incisor relationship.
Carry out an orthodontic assessment of this patient and then answer the following question:
Answers
Note that in the cases in whom URAs are advocated for interceptive treatment, it is assumed that the patient will have improved their oral hygiene to the necessary standard, that there is dietary control and that any carious lesions have been restored.
The rationale for the design of the appliances is detailed in Chapter 3 and is not repeated here. However, the reader is advised to review the relevant sections as appropriate.
Case 1
Orthodontic Assessment
This patient has a Class I skeletal pattern with average vertical proportions, no facial asymmetry, but mildly incompetent lips.
The patient is in the mixed dentition and has mild gingivitis around the LLS and some recession associated with LR1. There is also evidence of caries in some deciduous teeth and LR6 has previously been extracted.
The arches are well aligned except for the irregularity associated with UR1 and LR1, and the mild rotation of UL2 (disto-labial). The ULS and LLS are normally inclined clinically except for UR1 (retroclined) and LR1 (proclined).
In occlusion, the incisor relationship is Class I except for UR1 where the relationship is Class III. The overjet is within normal limits except for UR1 (−1 mm). The overbite is average and complete to tooth; the centre-lines are co-incident and correct. The lower centre-line is marginally to the right.
The buccal segment relationship is Class I on the left, but LR6 has previously been removed. There is a slight forward displacement on closure associated with UR1 and LR1.
Problem List
- Mild gingivitis and recession in the lower labial segment (LLS)
- Caries
- Mother concerned about crossbite and displacement of LR1
- Mandibular displacement
- Rotated UL2
- Crossbite of UR1
- Labially displaced LR1
Answers to Questions
Yes.
Rationale: The patient has a favourable skeletal pattern; there is a forward displacement on closure (the patient can make an edge-to-edge contact of UR1 with LR1), and the overbite will be favourable once the eruption of UR1 is no longer impeded by the occlusion and LR1 and LR2 are able to spontaneously align. The incisor inclinations are favourable and there is room to move the tooth.
It is important to note that prior to treatment starting, the patient and parent/guardian should be warned that the overjet may increase following correction of UR1 as the displacement is corrected. The mandible may therefore drop back as it no longer has to be brought forward (displaced forward) to ‘clear’ the instanding UR1.
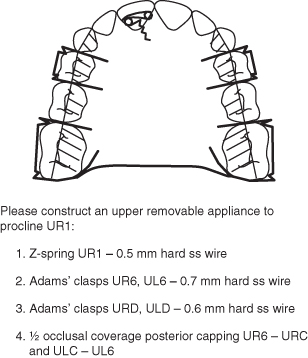
Appliance Design
A suggested design is shown in Figure 6.17.
Figure 6.17 Laboratory prescription for a URA to procline UR1 (Case 1).
Case 2
Orthodontic Assessment
The patient has a severe Class II division 1 malocclusion on a moderate Class II skeletal base with an increased lower anterior face height and an increased Frankfort–mandibular planes angle (FMPA). The mandible is symmetrical. The lips are incompetent and the naso-labial angle is average.
Intra-orally, the patient is in the late mixed dentition phase with both upper second primary molar teeth retained. The LLS is mildly crowded and of average inclination, and the ULS is also mildly crowded, but proclined.
In occlusion, the overjet is increased (10 mm) and the overbite is increased and complete to gingivae.
The buccal segment relationship is a full unit Class II on the molars and canines bilaterally. The upper centre-line is coincident with the facial midline and the lower centre-line is 1 mm to the right of the upper centre-line. There are no crossbites and no displacements.
Problem List
- Patient’s complaint: top teeth stick out
- Moderate skeletal Class II base
- Incompetent lips and lower lip trap
- Mild crowding of LLS
- Proclination of upper labial segment (ULS)
- Increased overjet
- Increased and complete overbite
- Class II buccal segment relationship
Answers to Questions
No.
Rationale: The patient has a mo/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


