Chapter 6
Permanent Dentition: Complicated Crown Fractures: Enamel-dentine-pulp Fractures, Enamel-dentine-pulp-root Fractures
Aim
To provide a review of current practice for the treatment of coronal fractures involving the pulp.
Outcome
After reading this chapter the reader should be aware of the appropriate treatment for fractures of the crown, and crown and root involving the pulp.
Aetiology
Complicated crown fractures, like the injuries described in Chapter 5, are commonly the result of falls, accidents involving bicycles and scooters, and contact sports, but with a greater impact force.
Diagnosis
These fractures are obvious but accurate diagnosis is critically important following thorough cleaning with moist gauze. Initial assessment for these injuries should include the clinical and radiographic parameters as outlined in the ‘trauma stamp’ in Table 1-1 and discussed in Chapter 1.
Treatment
The pulps of young permanent teeth, in particular those with incomplete apices, have a very rich blood supply. For this reason, immature permanent pulps have great healing capacity and generally respond well to treatment aimed at pulp preservation.
The most important function of the pulp is to lay down dentine which forms the basic structure of teeth, defines their general morphology, and provides them with mechanical strength and toughness. Dentine deposition commences many years before permanent tooth eruption and when a tooth erupts the pulp within still has work to do in completing root development. Newly erupted teeth have short roots, their apices are wide and often diverging, and the dentine walls of the entire tooth are thin and relatively weak (Fig 6-1a).
Provided the pulp remains healthy, dentine deposition and normal root development will continue for two to three years after eruption in permanent teeth (Fig 6-1b). One of the key goals of paediatric dentistry is therefore to protect and preserve the pulps of teeth in a healthy state, at least until tooth development is complete. Loss of pulp vitality before a tooth has reached maturity may leave the tooth vulnerable to fracture, and with an unfavourable crown-root ratio. Endodontic treatment of non-vital, immature teeth can also present technical difficulties, which may compromise the long-term prognosis of the tooth.
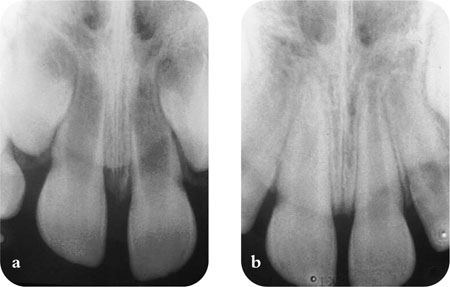
Fig 6-1a,b The maturation of the root takes at least 2–3 years after the eruption of the crown into the mouth.
When traumatic pulpal exposure occurs, a variety of chemical, physical, and microbial agents may act on the pulp directly or through the overlying porous, tubular dentine to cause irritation. Microbial invasion is by far the most serious. However, the radicular pulp has enormous capacity to remain healthy if all infected and inflamed coronal tissue is removed and an appropriate wound dressing and coronal restoration is applied. An untreated exposed pulp will eventually become non-vital and inflammation will spread through apical, lateral and furcal canals to affect the periradicular tissues.
The priority in enamel-dentine-pulp injuries involving immature teeth is the preservation of vital radicular pulp which will allow continued root growth. In the case of fully formed permanent teeth, there is still merit in preserving pulp vitality and avoiding pulpectomy if possible, although the regenerative capacity of the mature pulp may be limited. The injured pulp must be appropriately sealed from bacteria so that it is not infected during the period of repair. Pulp amputation by partial pulpotomy or complete coronal pulpotomy is often the treatment of choice but pulp capping can be considered in certain circumstances. The treatment for two diagnostic categories will be considered:
-
Enamel-dentine pulp fractures
-
Complicated crown-root fracture (involving pulp).
Enamel-dentine Pulp Fractures
Vital Pulp Therapy
-
Pulp capping
-
Pulpotomy
Non-vital Pulp Therapy
-
Pulpectomy
Vital pulp therapy – pulp capping
The procedure must be completed within 24 hours of the incident. No instruments should be inserted into the exposure site, and any bleeding should be controlled with sterile cotton wool. A blast of air from the three-in-one syringe will drive debris and microorganisms into the pulp. A layer of setting calcium hydroxide cement is gently flowed onto the exposed pulp and surrounding dentine quickly overlaid with a ‘bandage’ of adhesive material, e.g. compomer, pending definitive aesthetic restoration at a later date. A successful direct pulp cap will preserve the remaining pulp in health and should promote the deposition of a bridge of reparative dentine to seal off the exposure site. Research continues on alternative capping agents, including mineral trioxide aggregate (MTA), glass-ionomer cements and direct resin bonding, but calcium hydroxide coverage remains the most commonly recommended wound dressing in traumatic injuries.
Pulp capping – assessment and review
Review after a month, then three months and eventually at six-monthly intervals for up to four years to monitor pulp vitality. Periodic radiographic review should also be arranged to monitor dentine bridge formation, root growth, and to exclude the development of necrosis and resorption. On each radiograph check the following with reference to the previous radiographs:
-
root is growing in length
-
root canal is maturing (narrowing)
-
compare with antimere.
If growth is not occurring, the pulp should be assumed to be non-vital. See ‘Non-vital pulp therapy – Pulpectomy’.
Vital pulp therapy – pulpotomy
In pulpotomy, a portion of exposed vital pulp is removed to preserve the radicular vitality and allow completion of apical root development (apexogenesis) and further deposition of dentine on the walls of the root. Following trauma, this procedure is the treatment of choice in circumstances where the pulp has been exposed to the mouth for more than 24 hours.
Technique (Fig 6-2)
-
Under local anaesthesia pulp tissue is excised with a sterile diamond bur running at high speed under constant water cooling. This causes least injury to the underlying pulp and is preferred to hand excavation or the use of slow-speed steel burs.
-
Microbial invasion of recently-exposed vital pulp is usually superficial, and generally only 2–3 mm of pulp tissue needs to be removed (partial pulpotomy (Cvek)).
-
Excessive bleeding from the residual pulp which cannot be controlled with saline moistened cotton wool indicates that further excision is required to reach healthy tissue (coronal pulpotomy).
-
Gently rinse the wound with sterile saline an/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


