6
Orthodontically driven corticotomy: Tissue engineering to enhance the treatment, guided by the orthodontist
Federico Brugnami1 and Alfonso Caiazzo2,3
1 Private Practice Limited to Periodontics, Oral Implants and Adult Orthodontics, Piazza dei Prati degli Strozzi 21, Rome, Italy
2 Department of Oral and Maxillofacial Surgery, Boston University Henry M. Goldman School of Dental Medicine, Boston, MA, USA
3 Centro Odontoiatrico Salernitano, Via Bottiglieri 13, Salerno, Italy
Introduction
“Corticotomy facilitated therapy does not create anatomical fragments or separate ‘parts’. Corticotomies re-engineer physiology seek to re-engineer epigenetic potential in both the basic physiology of healing and ultimate morphogenesis at the molecular level of DNA and (endogenous and grafted) stem cells.” Tissue engineering is the sum of: “Tissue – a collection of cells for a common purpose” and “Engineering – marshaling natural forces and manipulating them to a predetermined design” (Williams and Murphy, 2008).
In the oral surgery and orthodontic literature, the term “corticotomy” is often confused with “osteotomy.” As described in Chapter 3, corticotomy is the cut of the cortices and osteotomy is the cut through the entire thicknesses, including the interposed medullary bone between the cortices, potentially creating a mobilized segment of bone and teeth. The confusion was mainly created because the earlier concept of rapid tooth movement was based on bony block movement in corticotomy techniques. Suya (1991) had proposed, in fact, that the tooth embedded within a block of medullary bone served as the handle by which the bands of less dense medullary bone surrounding the teeth were moved block by block. Unfortunately, this theory is still influencing surgeons in attempting to design a block of bone, therefore including buccal and lingual vertical and sub-apical full-thickness horizontal cuts circumscribing the roots of the teeth, as it would be done in osteo-distraction cases. The Wilckos were the first to demonstrate that the movement does not result from repositioning of tooth–bone blocks (Figure 6.1), but rather from a cascade of transient localized reactions in the bony alveolar housing leading to bone healing (Wilcko et al., 2001).

Figure 6.1 The Wilckos were the first to demonstrate that the movement does not result from repositioning of tooth–bone blocks.
The historical background and the development of the surgical technique is described in Chapter 1. For the purpose of this book we will consider the work of the Wilcko brothers as the renaissance of modern corticotomy. They started to work in the early 1990 on a combined surgical–orthodontic therapy with an innovative technique of combining corticotomy surgery with alveolar grafting. They initially termed their technique Accelerated Osteogenic Orthodontics® (AOO®) and more recently changed the terminology to Periodontally Accelerated Osteogenic Orthodontics® (PAOO®) (Wilcko et al., 2001). In this chapter and mainly in the rest of the book the term corticotomy and PAOO® may be used synonymously.
Surgical techniques: the beginning of tissue engineering in orthodontics
As described in previous chapters, corticotomy was originally planned as an in-office alternative to orthognathic surgery, which is quite invasive, technical demanding, time consuming, and not so friendly for the patient (Köle, 1959). During the following years, and especially after Suya’s (1991) publication, the surgery was modified to make it gradually less invasive and comparable to a full-mouth periodontal surgery (Wilcko et al., 2001). More recently it has been modified to the point that it can be done in a flapless fashion (Dibart et al., 2009). Regardless of the type of surgical approach that made the procedure more and more applicable and acceptable for the patient, the major shift has been made on the rationale of the technique. Thanks to the work of the Wilcko brothers and their PAOO® technique, corticotomy became a tool not only to speed up orthodontics, but also to enhance it. Adding a bone graft to the area of decortication allowed a profound modification of the alveolar basis and exceptionally boosted the treatment options (Wilcko et al., 2001). It was the start of a concept that is leading toward bone engineering to modify and mold the alveolar basis, stretching the limits of orthodontic treatment. Corticotomy offers the following advantages: the possibility of solving crowding without the need for routine extraction of premolars; a more robust periodontium, and therefore a lesser risk of periodontal damage; less risk of root resorption; wider movements; less relapse; the possibility to correct transverse and mild sagittal discrepancy, modify differential anchorage of teeth, and the ability to modify the lower third of the face (Wilcko et al., 2003). In other words, it exponentially expanded the scope of orthodontics and the limits of safe orthodontic treatment, and the speed merely became a marketing bonus to enhance patient acceptance. The treatment was, yes, much faster than the traditional one, but speed was overtaken by the other advantages.
Single-flap corticotomy
In the previous chapters, two major distinct surgical approaches have been described: the original one, described by the Wilcko brothers, namely, PAOO® (Wilcko et al., 2001); and the most notable modifications described by Dibart et al. (2009), named Piezocision®. The Wilckos’ approach is classically contemplating a full-mouth, full-thickness flap elevation, both in the vestibular and palatal/lingual side with or without bone graft, and it is generally involving the entire dentition in both jaws. In the Piezocision® approach, the regional acceleratory phenomenon (RAP) is started in a flapless fashion, with the surgical insult being carried out with a piezoelectric scalpel through incisions of the mucosa. (For a more comprehensive description of the techniques, please refer to Chapters 1, 3, and 5.)
We would like to introduce a third surgical approach that we routinely use in corticotomy treatment, which is a slight modification of the PAOO® protocol. This involves only a single full-thickness flap elevation in the anticipated direction of the orthodontic movement. This is, normally, a vestibular flap, and we term it single-flap corticotomy (SFC). For example, for de-crowding, which is one of the most common types of orthodontic problems where corticotomy is used (Brugnami et al., 2010), only the vestibular flap is elevated. For arch expansion, the same approach would be utilized. On the other hand, if a lingualization is planned, a single flap on the lingual side can be performed (Figure 6.2).
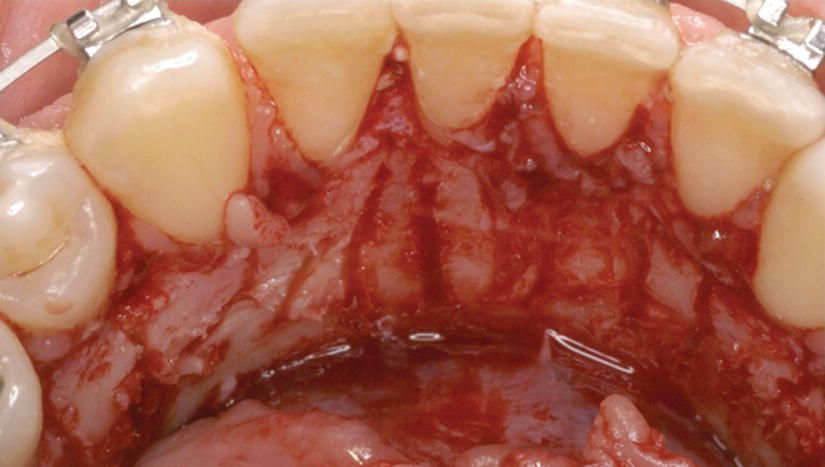
Figure 6.2 Lingual approach in the SFC technique.
Surgical technique
Since the surgical technique used is very similar to the one described in Chapter 3, only the small differences will be outlined here. Cone-beam computed tomography (CBCT) scans become critical, depending on the type and entity of movement and the periodontal biotype, in evaluating three-dimensional (3D) alveolar bone morphology and the indications for corticotomy and bone grafting. If the anticipated movement is beyond the alveolar bone surrounding the tooth (i.e., expansion or proclination) and/or the bone is <1 mm, the combination of corticotomy and bone graft is strongly suggested.
Incision design. In SFC, only one flap is elevated by definition. In most cases it is also segmental and performed only in the area where the anticipated movements will take place. It is comparable to periodontal surgery, where rarely one arch is treated simultaneously, but rather in quadrants or sextants fashion. The incision will be influenced accordingly. In most cases we may need to place vertical releasing incisions to avoid periodontal involvement of teeth in the area where corticotomy would not be performed and to increase flap mobility. The vertical incisions may be placed at least one tooth and a half away for the most mesial and the most distal area where corticotomy is going to be performed. Intra-sulcular incision is carried out with a no. 15 Bard-Parker surgical blade. In adult patients with thin periodontium, a papilla preservation approach may be used so that the base of the papilla will not be elevated. Therefore, the horizontal incision will run at the base of the papilla, from the mesial line angle at the cemento-enamel junction of one tooth to the distal line angle of the contiguous one. Vertical incisions and periosteal undermining at the base of the flap are also useful for mobilization, positioning of the graft, and tension-free closure of the flap, as recommended in Chapter 3.
Flap reflection and exposure. Same as Chapter 3.
Corticotomy/surgical decortication. Authors suggest a combination of rear-vented high-speed, rotary surgical instrumentation under copious irrigation for speed and outlining of corticotomy (Figure 6.3) and a piezoelectric scalpel for refinement and small interproximal corticotomies, especially in the presence of root proximities (Figure 6.4). Some authors suggest that the piezoelectric scalpel may be superior to burs in terms of postoperative swelling (Sivolella et al., 2011). On the other hand, others have shown a higher increase in temperature and increase in surgical length compared with rotative instruments (Maurer et al., 2008). Thus, to date, there is no definitive evidence that piezoelectric scalpels are comparable or superior to classical rotary instruments (Cassetta et al., 2012), merely becoming a choice of the surgeon. In the flapless approach, a piezoelectric scalpel, for example, becomes much more practical and safe for the surgeon compared with a rotating bur (Figure 6.5).
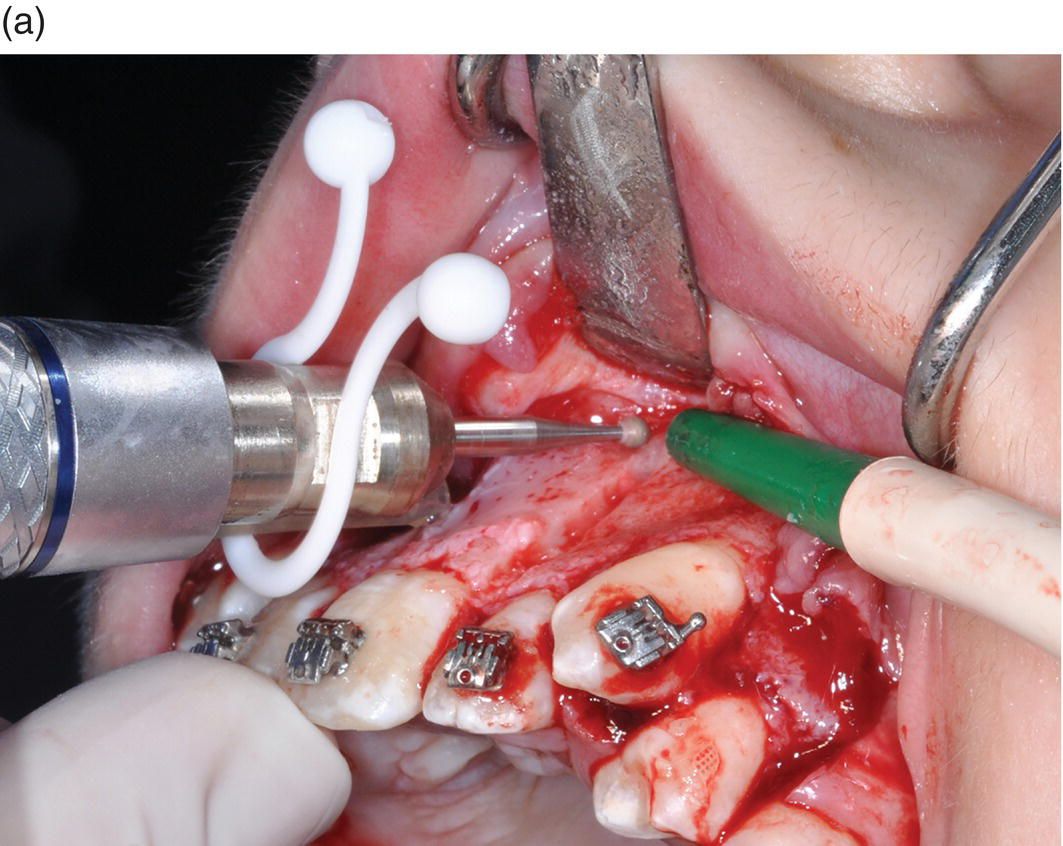
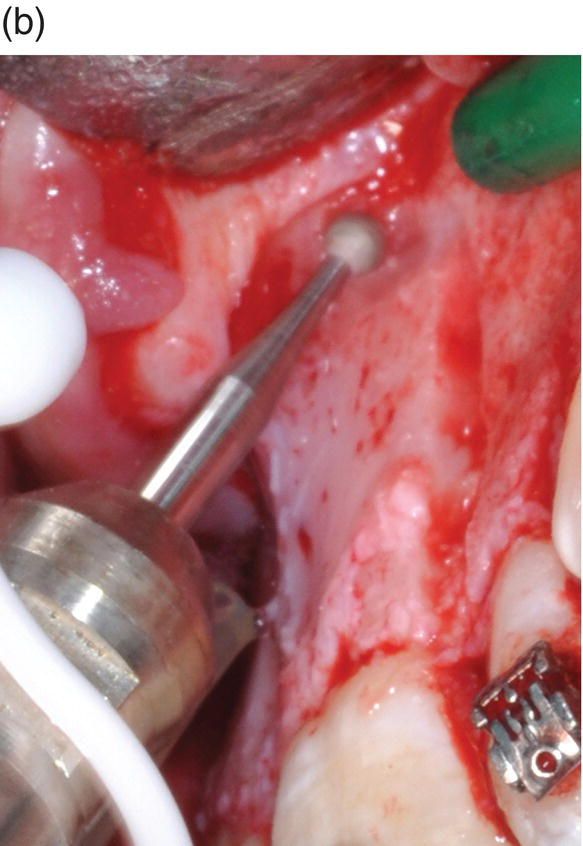
Figure 6.3 Use of rotatory instrument under copious irrigation in corticotomy: (a) for initial and faster corticotomy design; (b) close-up of a rotatory instrument used for initial corticotomy.


Figure 6.4 Use of piezoelectric scalpel: (a) refinement of initial corticotomy; (b) interproximal corticotomies, especially in the presence of root proximities.
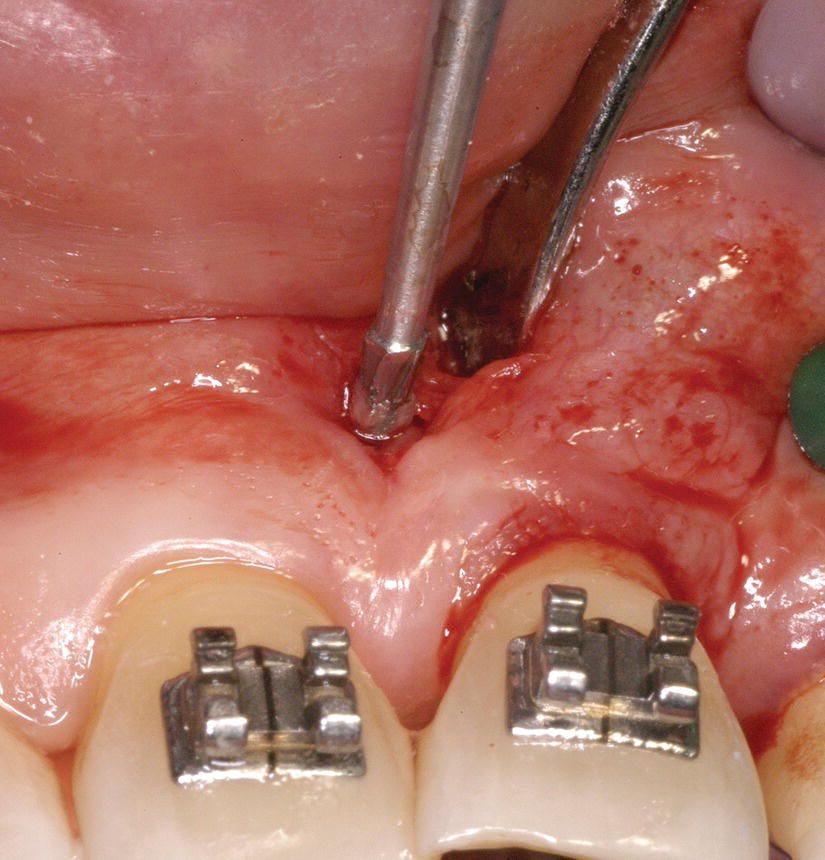
Figure 6.5 The use of rotatory instruments is less indicated than a piezoelectric scalpel in a flapless approach because the risk of soft tissue’s tearing.
The design of decortication is not relevant, but we try to overcome the fact that we do not elevate both flaps by deepening the interproximal cuts of at least 3 mm in the bucco-lingual direction and being at least 3 mm from the level of bone crest in the apico-coronal direction. We also perform a thinning of the alveolar bone surrounding the tooth in the anticipated direction of movement (Figure 6.6). This is an important part of the corticotomy, often ignored and difficult to perform in a flapless fashion (Piezocision®).
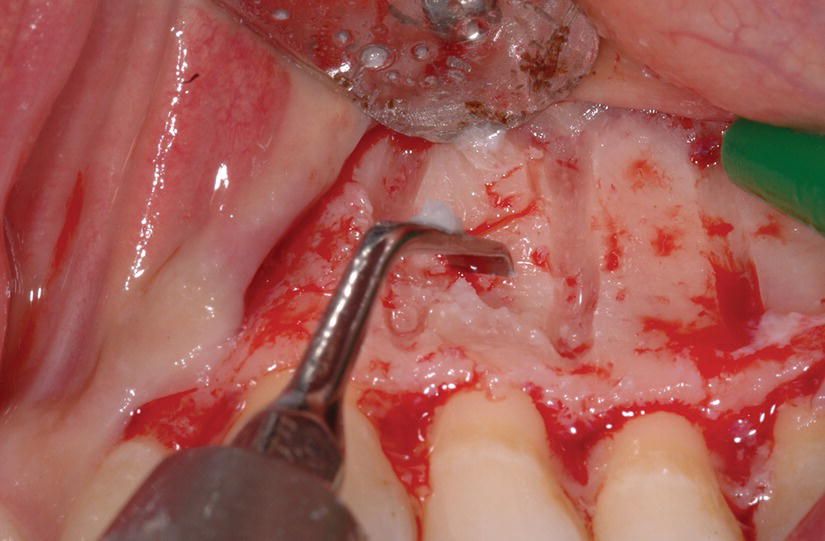
Figure 6.6 Thinning of the alveolar bone surrounding the tooth in the anticipated direction of movement.
Bone grafting and membrane. The use of bone grafting has already been widely discussed in Chapter 3. In grafting selection, slow resorption bovine xenograft or freeze-dried allograft are preferred (Figure 6.7). Autogenous and demineralized freeze-dried bone graft, which are more rapidly resorbed, should be avoided, unless utilized with a membrane and/or in layers with slow resorbing grafting material acting as a membrane (see Chapter 7). Calcium sulfate and other quick resorbing material should also be avoided, since they have shown a limited stability even in a short period of time (Figure 6.8).

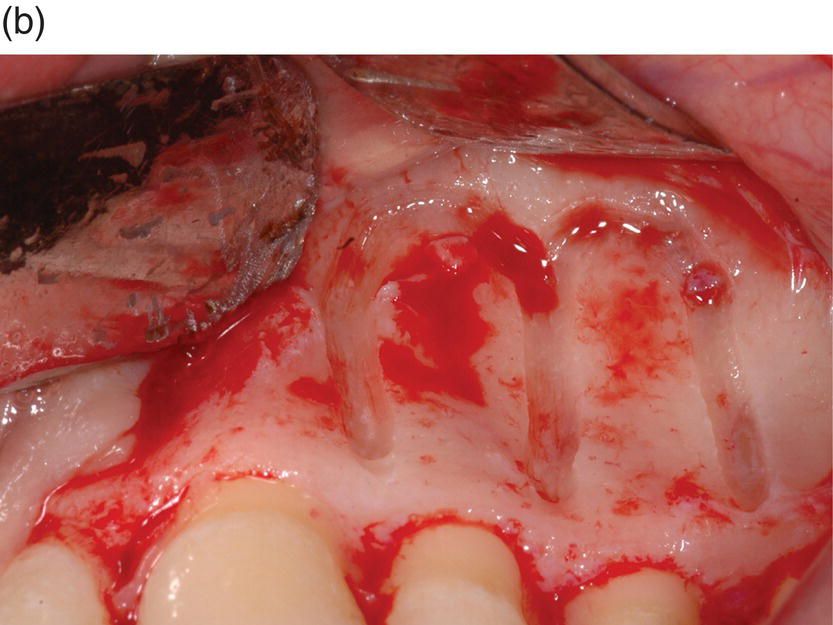

Figure 6.7 Application of a xenogeneic grafting material at the corticotomy site: (a) flap elevation and bone exposure on the corticotomy site; (b) corticotomy design; (c) application of a xenogeneic graft material on the site of corticotomy.


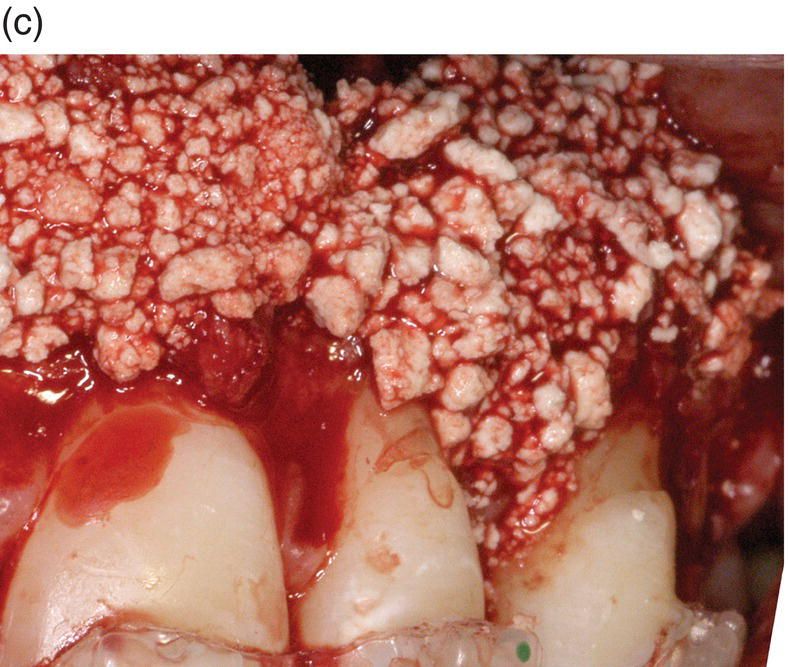
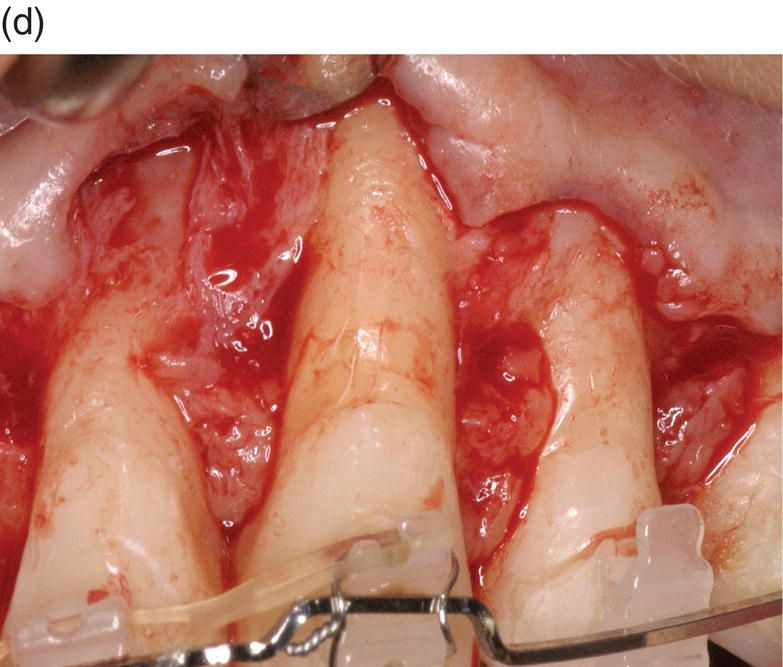
Figure 6.8 Fast resorbing grafting materials should be avoided in corticotomy: (a) flap elevation and bone exposure; (b) autologous bone graft in place; (c) application of calcium sulfate grafting material; (d) at 3 months post operation, a connective tissue graft was requested to correct a muco-gingival problem, created by persistent prolonged inflammation in the area of grafting. After elevation of the flap, no signs of grafting or regeneration were present; actually, the level of bone was worse than the pre-operative level.
The volume of the graft material used is dictated by the direction and amount of tooth movement predicted, the pretreatment thickness of the alveolar bone, and the need for labial support by the alveolar bone.
Lingual and buccal plates are very thin close to the margin. An inclination of the tooth will produce a stress and a potential resorption at the marginal cervical level in the direction of the rotation and at the opposite apical side. It is important, therefore, to try to deliver the bone graft where the bone is thinner and where the anticipated movement will produce the resorbing stress.
For these reasons, a tunnel approach to grafting is not suggested, since it is very difficult to place the graft under the attached gingiva and the graft has the tendency to be displaced too apically (Figures 6.9 and 6.10).
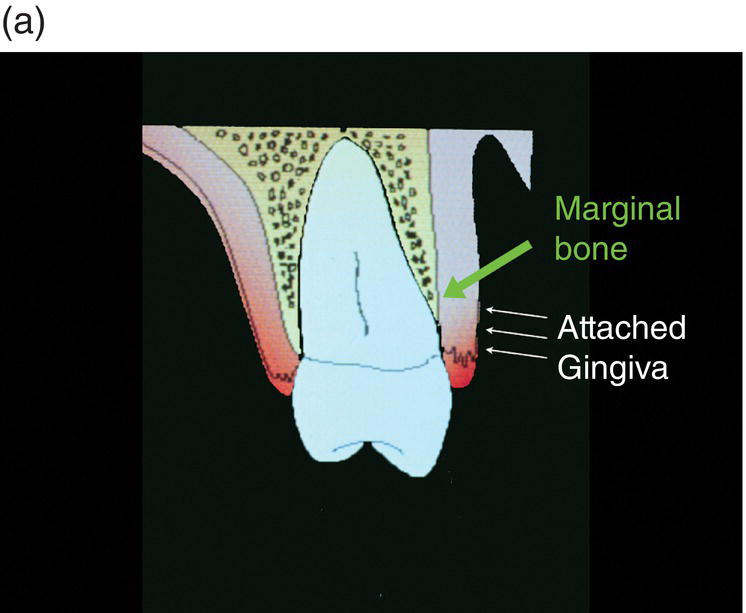
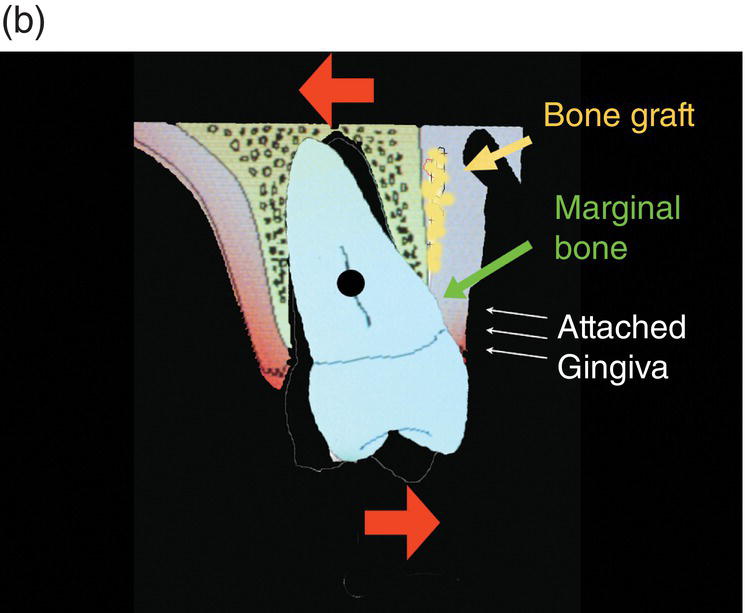
Figure 6.9 (a) The volume of the graft material used is dictated by the direction and amount of tooth movement predicted, the pre-treatment thickness of the alveolar bone, and the need for labial support by the alveolar bone. (b) In the case of tooth inclination, it would be useful to place the bone graft as close as possible to the cervical bone margin. A tunnel approach has a tendency to displace the graft too apically, far from the anticipated resorptive stress caused by the orthodontic movement, which in case of inclination would be at the marginal level in the direction of the inclination and at the apical level on the opposite side.
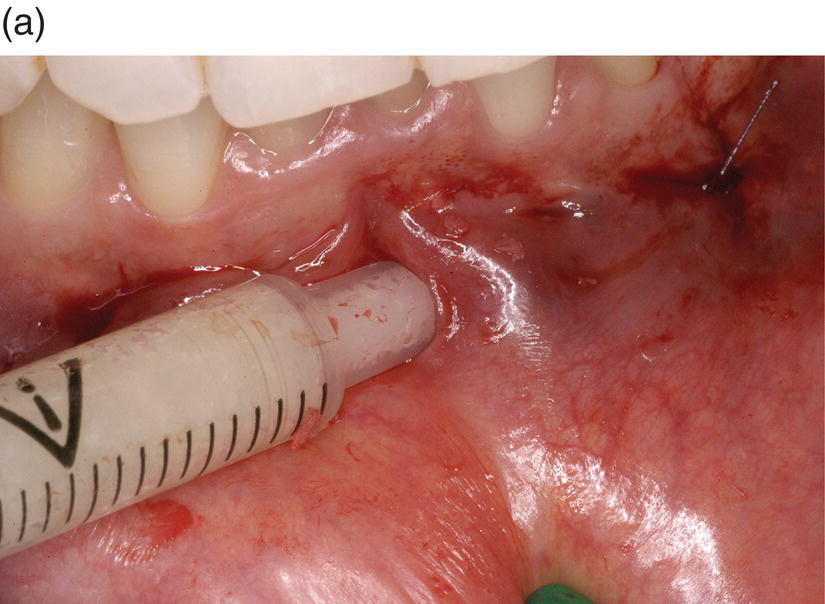
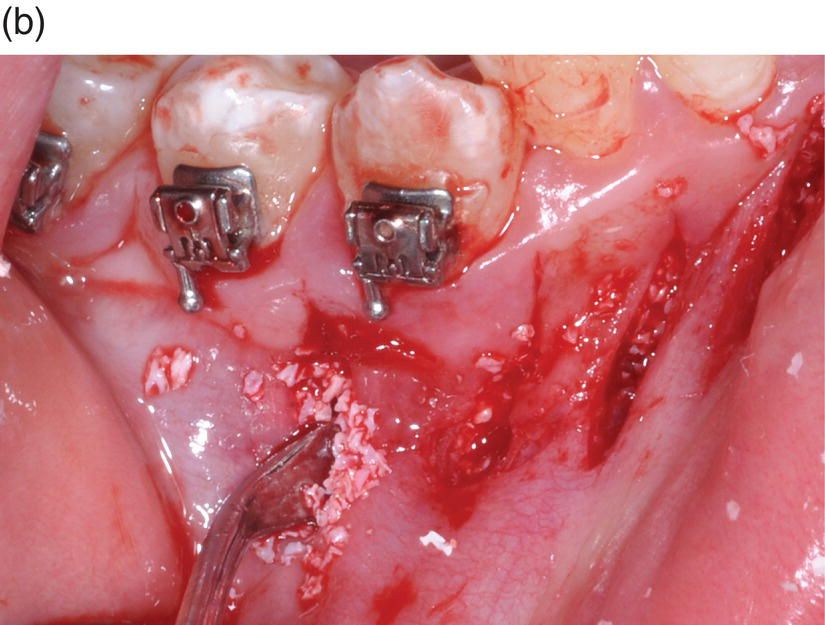

Figure 6.10 In some cases a tunnel approach to grafting is not suggested, since it is very difficult to place the graft under the attached gingiva and the graft has the tendency to be displaced too apically: (a) insertion of grafting material with a syringe into the tunnelized flap; (b) positioning of the grafting material by means of a thin periosteal elevator; (c) 10 days follow-up in a different case – note the bulk of the graft material, positioned below the muco-gingival line.
Since, as already described, most SFCs are done in sextants or quadrants, the mobility of the flap may be inferior compared with a full arch design, when elevation has been carried out as described in Chapter 3. This is somehow limiting the quantity of bone graft we can deliver (0.5 cm3 for approximately three or four teeth) and being still able to achieve a tension-free reapproximation of the flap. We often try to overcome the lesser volume of graft by following the principle of guided bone regeneration (GBR) and place a resorbable, collagen membrane over the graft (Figure 6.11).
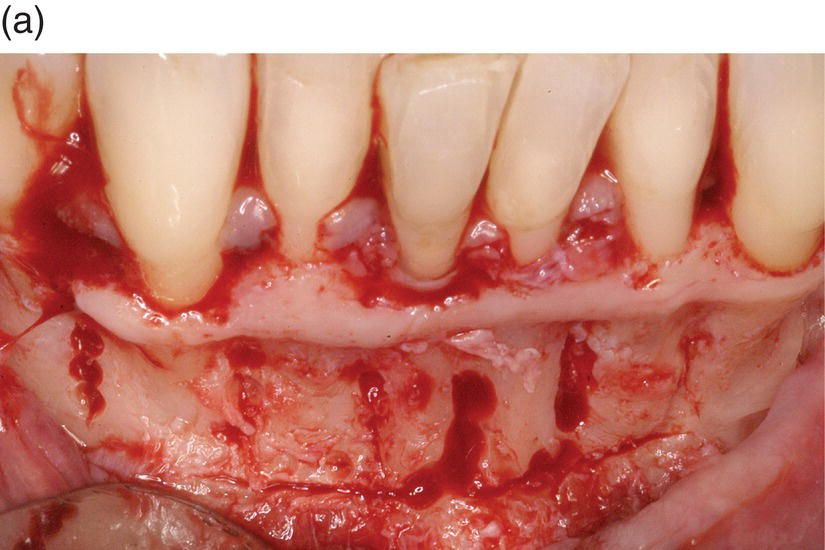


Figure 6.11 Since most SFCs are done in sextants or quadrants, the mobility of the flap may be inferior compared with a full arch design. This is somehow limiting the quantity of bone graft we can deliver (0.5 cm3 for approximately three or four teeth) and being still able to achieve a tension-free reapproximation of the flap. We often try to overcome the lesser volume of graft by following the principle of GBR and place a resorbable, collagen membrane over the graft. (a) Flap elevation and bone exposure. (b) Application of the grafting material. (c) Collagen membrane positioning.
Care should be taken to avoid fixation pins, which may interfere with orthodontic movements (Figure 6.12).
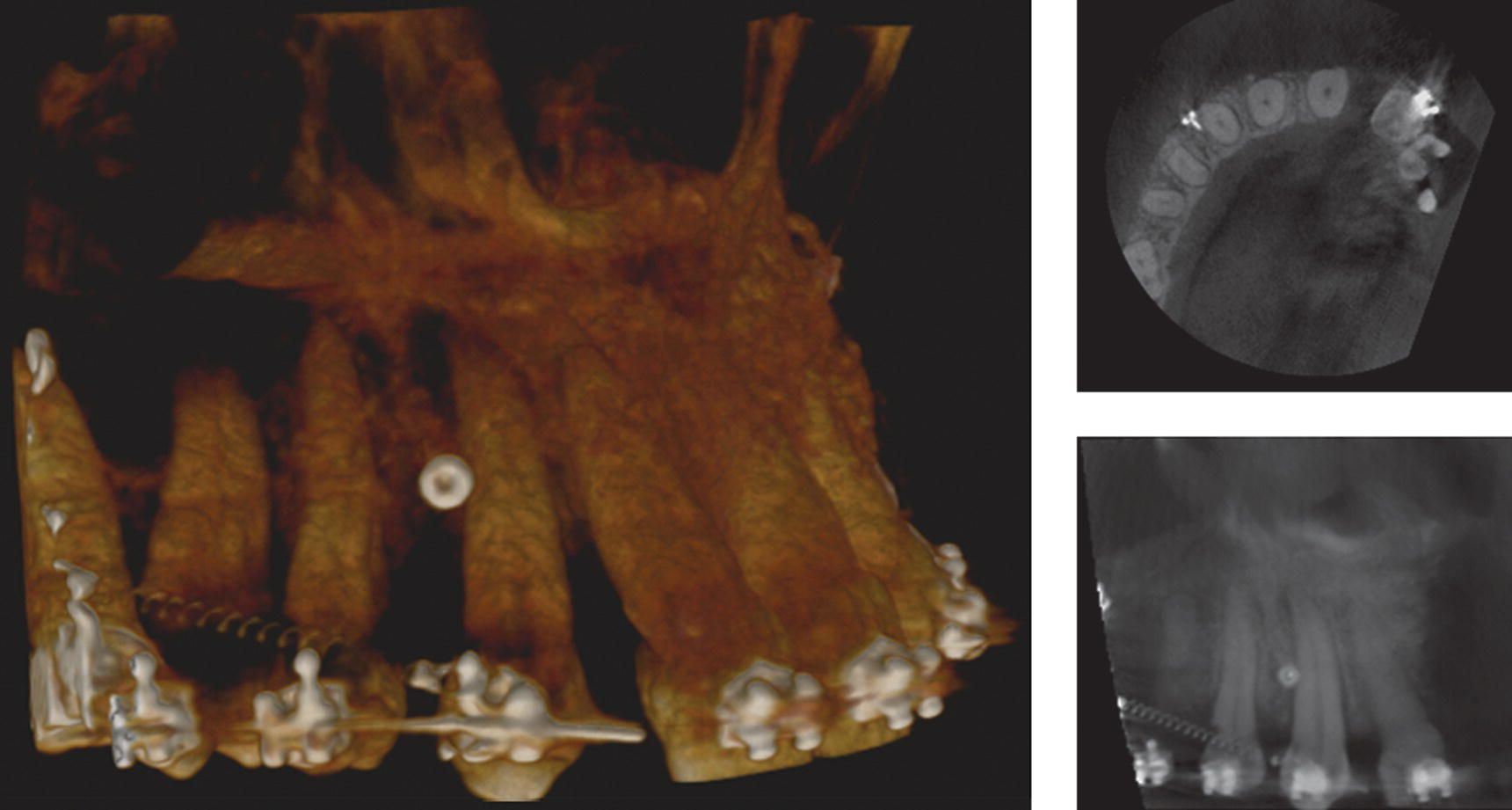
Figure 6.12 Fixation pins may interfere with tooth movement and should be avoided to fix the resorbable membrane.
A membrane will also enhance the possibility of true bone regeneration, compared with a fibro-encapsulation of at least the most superficial layers of the graft.
Only in those rare cases where thickness of cortical plates in the direction of movements is more than 2 mm and the entity of anticipated movement is very limited can bone grafting be avoided.
Suture and postsurgical considerations. Resorbable sutures (4-0 or 5-0 vicryl) are recommended for suturing. Post-operative instructions include oral antibiotics (7–10 days) only if bone graft is used and chlorhexidine 0.2% b.i.d. rinsing for 2 weeks. Pain medication is prescribed twice a day and used as required. Although swelling is anticipated, it may be extremely variable and seems to be due to the extent of the surgery (i.e., full arch versus sextant) or the type of flap elevation (flapless versus one flap versus both flaps) rather than the type of instrument used to perform corticotomies (round burs versus piezoelectric scalpel). An in-office retrospective examination also indicates that most of the patients will stop the analgesic before the second post-operative day, and only a very minor percentage continued for more than 4 days. Liquid diet should be followed for 1 week postoperatively and then a soft diet until suture removal, which normally takes place 1–2 weeks after surgery. Rapid orthodontic treatment is initiated immediately. The segmental and/or sequential approach to the surgery allows multiple surgery in sextants according to the orthodontic treatment plan (that is why we call it “orthodontically driven corticotomy” (ODC)). Contrary to the “classical” Wilcko technique and surgical design, it is, in fact, not mandatory to combine different mechanics to take as much advantage as possible of the RAP. It will be the RAP that will be initiated according to the orthodontic treatment plan. The segmental approach also amplifies the duration of the RAP. Being in fact performed when the actual orthodontic movements take place according to the orthodontic treatment plan and mechanics, the 4-month window of opportunity is not wasted while correcting other problems.
PAOO® versus Piezocision® versus single-flap corticotomy
Do we need another surgical approach? And how do we choose when to apply one technique over the others? We would like to answer that in this section, underlining the fact that most of the following considerations come from our clinical experiences and small retrospective analysis, and therefore they should not be taken as conclusive evidence. We would like to see some of our considerations validated or refused in an experimental model sooner or later, but for the time being this is what it is: not more than clinical experience and empirical observations and some retrospective analysis on a small pool of patients. The quest for the most minimally invasive technique that still does the job is not over yet. Although the concept of a very minimal surgical technique is somehow attractive, if this does not accomplish the goal then it becomes a useless tool. In our experience, the PAOO® approach is a long in-office procedure that may require up to 3 hours, and although generally well tolerated by the patients may be tedious. It also forces the orthodontist to make the majority of movements in a short period of time. As we know, the window of opportunity is, in fact, limited in time and may require the orthodontist to combine different mechanics in order to take advantage of the RAP. For example, in a treatment of a class II case, with anterior crowding and transverse discrepancy, it may be necessary to combine the wire mechanics to other appliances, such as a distalizer or a palatal expander. In other words, once the surgeon is done with a single-shot surgery, the orthodontist is trying to keep up with the window of opportunity and modify the treatment planning accordingly.
On the other hand, a Piezocision® approach could be feasible for the decrowding phase, but can be less predictable in mesio-distal bodily movements or traverse expansion. Most of the time a thinning of the bone toward the direction of movement is required and a simple cut in the interproximal bone may not be sufficient. The large amount of demineralization and the superiority of the piezoelectric surgery is far from being widely accepted and demonstrated (Sivolella et al., 2011). The most salient advantages compared with conventional techniques are selective cutting of hard tissue and a gentle and precise cut without the need for excessive force. This device does not harm the surrounding soft tissues, which makes it especially suitable for surgery in areas adjacent to vulnerable structures, such as blood vessels, nerves, and the meninges. Still, it has to be used with caution, since damage may eventually occur in the hands of careless surgeons. A clear disadvantage in clinical routine use is the longer time required for osteotomies (Schaller et al., 2005).
Research experience
Statement of the problem
Recently, PAOO® or SFC and Piezocision® have been proposed as an effective tool to accelerate orthodontic treatment. However, no previous reports exist comparing the differences between PAOO®/SFC and Piezocision®. We aimed to define specific indications on when the use of one technique is indicated over the other.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


