6
Lingual and Palatal Arches
Incisor Liability and Leeway Space
In the mixed dentition, the discrepancy between the mesiodistal widths of the smaller primary and larger permanent incisors averages approximately −7.4 mm in the maxillary arch and −5.1 mm in the mandibular arch (Moorrees and Chadha 1965). This discrepancy, called incisor liability, is one of the reasons why mixed-dentition patients experience crowding of the larger permanent incisors as they erupt. The other major reason for crowding is inadequate growth in the size of the alveolar arches in relation to the size of the permanent teeth.
In the posterior segments of the mixed dentition, the discrepancy between the mesiodistal widths of the larger primary canines and molars and the smaller permanent succedaneous canines and premolars, called the leeway space, averages approximately 2.4 mm in the upper arch and 4.3 mm in the lower arch (Moorrees and Chadha 1965). The leeway space can be used to align crowded incisors in many patients.
Passive Lower Lingual Holding Arch
A passive lower lingual arch can be placed in mixed-dentition patients who exhibit mild incisor crowding and have adequate leeway space to accommodate the erupting permanent teeth. Passive lingual arch therapy helped resolve up to 5 mm of lower incisor crowding (Brennan and Gianelly 2000). They reported that 60% of 107 patients who have an average of 4.85 mm of incisor crowding finished treatment with adequate arch length. The passive lingual arches lost an average of 0.4 mm of arch length during the course of the entire treatment. Another study found that lower incisor alignment remained stable for 9 years postretention in 76% of a group of mixed-dentition patients treated with a passive lingual arch (Dugoni, Lee, Valera, and Dugoni 1995). The evidence from these studies strongly supports the use of passive lower lingual holding arches as effective interceptive and preventive appliances in mixed-dentition patients who have minimal total arch length deficiencies.
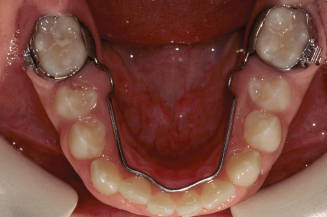
Mixed-dentition analyses like the Iowa or revised Hixon-Oldfather analyses are essential tools that help a clinician identify patients who have minimal total arch length deficiency and who can benefit from the placement of a passive lower lingual arch (see Chapter 5). For example, mixed-dentition patients with mild incisor crowding who are predicted by an analysis to have some excess of total arch length can benefit from passive lingual arch therapy. A patient with mild incisor crowding in the mixed dentition had a predicted total excess of 0.2 mm (Figs. 6.1 and 6.2). A lower lingual holding arch was placed in the patient’s mouth; his lower arch is shown in Figure 6.2 after the permanent canines and premolars had erupted. The patient illustrated in Figure 6.1 had a Class I occlusion; however, the same principles apply to patients with Class II and Class III malocclusions.
Figure 6.1. Iowa mixed-dentition analysis predicted an excess of 0.2 mm in the lower arch of this patient.

Figure 6.2. Lower lingual arch was placed and is shown after the eruption of the permanent canines and premolars.

Prevalence of Incisor Crowding
The U.S. Public Health Service surveyed the incidence of incisor irregularity in a large sample of whites, blacks, and Mexican Americans from 1988 to 1991 (Tables 6.1 and 6.2) (Brunelle, Bhat, and Lipton 1996). About 25% of the sample had excellent incisor irregularity scores (a score of 0). About 20% of U.S. citizens between 8 and 50 years of age had incisor irregularity scores or 5 or greater. The remaining 55% of the population had incisor irregularity scores between 1 and 4. Unfortunately the Incisor Irregularity Index (Little 1975) does not directly correspond to the tooth size–arch length discrepancy (TSALD) measurement; nevertheless, we can probably assume a large number of the children with alignment scores between 1 and 4 can potentially benefit from appropriately timed placement of a lower passive lingual holding arch.
Table 6.1. Incisor Irregularity Scores in Americans 8–50 Years Old
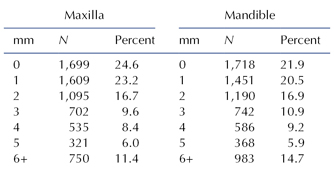
From Brunelle, Bhat, and Lipton (1996).
Table 6.2. Incisor Irregularity Index Scores by Age, Gender, and Race of Americans Ages 8–50 Years Old1
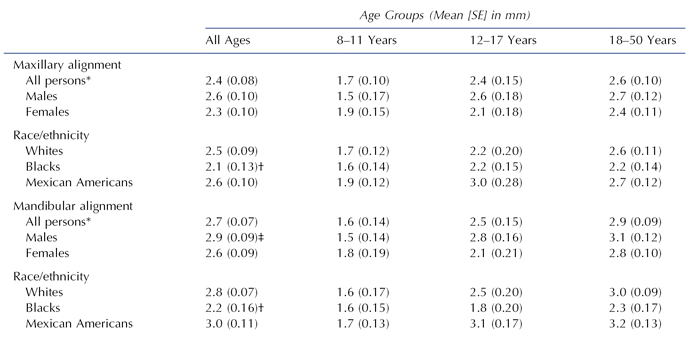
*Includes persons of “other” race/ethnicity designations.
†Blacks are different from whites and Mexican Americans, p ≤ 0.01.
‡Males are different from females, p < 0.01.
1From Brunelle, Bhat, and Lipton 1996.
Table 6.2 summarizes the mean Incisor Irregularity Index scores by age, gender, and race in the maxilla and the mandible. Blacks had higher mean Incisor Irregularity Index scores than whites and Mexican Americans in upper and lower arches. In the mandibular arch, females had significantly lower irregularity scores than males.
Premature Loss of a Primary Molar
Mixed-dentition patients who have crowding due to larger teeth and shorter and narrower arches are more susceptible to premature loss of a primary molar than are those who have adequate arch length and width to accommodate the permanent teeth (Ronnerman and Thilander 1978). Normal eruption may occur in children who lose a primary molar prematurely but who also have adequate arch lengths and widths.
To preserve needed arch length and prevent unnecessary crowding complications in those patients who have minimal to moderate crowding problems, clinicians must insert a passive lingual or palatal holding arch after the premature loss of a primary second molar. Premature loss of a primary first molar in the lower arch should also prompt the placement of a lower lingual arch in these patients (Northway 2000). If the unilateral premature loss of a primary molar is ignored, it may result in a bilateral asymmetry in arch length, leading to an asymmetric malocclusion in the permanent dentition. Intervention in the mixed dentition with a lingual or palatal holding arch may prevent the need for future orthodontic treatment or reduce the severity of a malocclusion.
A patient who lost his primary lower second molars is shown in Figures 6.3 and 6.4. Shortly after the loss, a lower lingual holding arch was placed (Fig. 6.3). Orderly eruption of the permanent premolars is illustrated in Figure 6.4.
Figure 6.3. Loss of both primary second molars in a patient with minimal arch length deficiency prompted placement of a holding arch.

Figure 6.4. Lower arch after eruption of the second premolars.
Asymmetric Loss of a Primary Canine
Patients who have an incisor liability and inadequate arch length in the anterior part of their arches often experience the asymmetric loss of a primary canine. As the permanent lateral incisors try to erupt, one of them can stimulate the resorption of the root of a primary canine. The unilateral loss of the canine not only provides arch length for the eruption of the lateral incisor but also causes a shift in the dental midline to the side of the lost canine. Clinicians who observe the early stages of this phenomenon can often prevent the midline shift by extracting the remaining primary canine. Once the dental midline is shifted away from the facial midline, the permanent teeth in the anterior part of the arch will retain this asymmetry. Intervention in the mixed dentition with a fixed appliance can correct the already shifted midline. The retained primary canine must be extracted to accomplish the treatment. The corrected lower incisors are retained with a passive lower lingual arch that has spurs soldered on the wire to keep the incisors from shifting laterally until the permanent canines erupt. A Hawley retainer with wires on the distal surfaces of the lateral incisors is used to retain the corrected incisors in the upper arch.
A patient with an ectopically erupted lower right lateral incisor that exfoliated the lower right primary canine is shown in Figures 6.5 through 6.8. The patient’s lower dental midline had shifted 2 mm to the right of the facial midline. The maxillary dental midline was 1 mm to the left of the facial midline. His mixed-dentition analysis predicted an excess of 0.9 mm on the lower right side and 5.1 mm on the lower left side. In Figure 6.6, the edgewise fixed appliance used to correct the midline and align the lower incisors is shown. A lower lingual arch with soldered spurs, shown in Figure 6.7, was cemented after the incisors were aligned. Figure 6.8 shows coincident upper and lower dental midlines following phase 2 comprehensive orthodontic treatment of this patient during his adolescent years.
Figure 6.5. Ectopic eruption of the lower right lateral incisor forced the exfoliation of the right primary canine.

Figure 6.6. After extraction of the left primary canine, the lower incisors were moved leftward and centered on the lower arch.

Figure 6.7. Lower lingual arch with spurs to hold the incisors from drifting is viewed when the spurs needed removal and the wire adjusted to allow eruption of the left first premolar.

Figure 6.8. Teeth are seen after a fixed appliance, used in phase 2 treatment, was removed. The dental midlines were coincident.

Nance Holding Arch
The Nance or palatal holding arch consists of two bands on the upper first molars connected by a wire with an acrylic pad that rests on the anterior palate. This passive appliance is used to maintain upper arch length when premature loss of a primary molar occurs or when maintenance of arch length is desired in a patient who has borderline arch length deficiency.
A patient who prematurely lost her upper right primary second molar is shown in Figures 6.9 through 6.12. Her upper right first m/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


