Chapter 5
Entering “Calcified” Systems
Aim
To describe common age changes which complicate pulp access and introduce methods which may assist entry.
Outcome
After studying this chapter, the reader should have greater understanding of changes which complicate entry to the aged tooth, and be conversant with a variety of techniques which may assist orientation and entry.
The Frustration of the “Calcified” Pulp
Entry to canal systems can be difficult. Most dentists know the frustration of the “calcified” tooth (Fig 5-1), a common finding in heavily restored teeth in ageing populations. Regrettably, such teeth are not immune to apical periodontitis. Compromise, referral or extraction are often the only solutions in practice.

Fig 5-1 Facing a brick wall! The calcified pulp system of a middle-aged patient.
Pulp space diminishes by:
-
reduction of pulp chamber and canal volume
-
calcified deposition within the chamber and canals.
These changes can present alone or in combination.
Reduced Chamber and Canal Volume
Pulps continue to secrete dentine throughout life. In molars, this is mainly on the floor and roof of the chamber, converting it from a deep cavern to a flat disc (Fig 5-2a,b). This process also narrows the entrances and moves them closer to the centre of the tooth.
Incisor and canine pulps retreat out of the crown and centrally (Fig 5-2c,d).
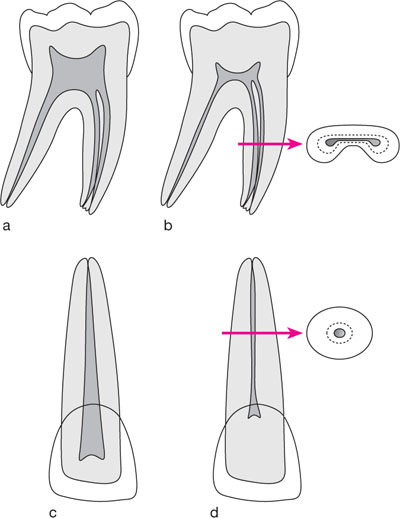
Fig 5-2 Age changes in pulp volume.
(a) Molar pulp system in a young adult. (b) Dentine deposition on the chamber roof and floor converts it to a flat disc which is easily traversed without realising by a poorly orientated bur. The first “give” can be the furca! The canal entrances also narrow and move centrally, whilst in cross-section, the canals narrow concentrically. (c) Incisor pulp system of a young adult. (d) Retreat of the coronal pulp apically and centrally. In cross-section, the root canal again narrows concentrically.
The picture in the crown can be complicated by irregular “irritation” dentine, secreted to wall off tubules exposed by caries, dentistry and wear (Fig 5-3).

Fig 5-3 Irregular, irritation dentine laid down to wall-off tubules opened by caries.
In roots, dentine deposition is always concentric. When searching and probing for the pulp in a root, it can only be in the centre of the mass of dentine which it formed (Fig 5-2b,d).
What About Apical Calcification?
Failure to reach length in a canal is often blamed on apical calcification. In truth, canals do not suddenly calcify in their apical reaches, and are more commonly wider in this protected apical region than further coronally where external irritants can provoke dentine deposition. Deep obstructions usually represent:
-
impacted debris
-
compacted pulp tissue
-
abrupt canal curvatures, often in a plane which is not visible in normal radio-graphic views.
The illusion of apical calcification can also arise as tapered instruments are advanced into canals with parallel or coronally narrowed walls (Fig 5-4). The interference actually lies coronally, causing the instrument to hang-up, making apical progress difficult, and rationalised in the mind of the operator as an apical blockage.
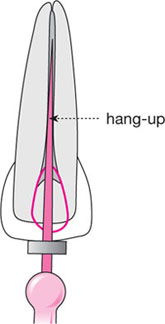
Fig 5-4 Hang-up of a file giving the illusion of apical obstruction. Opening the canal coronally allows the file to drop deeper.
Calcified Inclusions
Islands of calcification form around degenerating blood vessels and nerve fibres in the pulp. These glassy translucent deposits are not strictly dentine, and can appear very dense on radiographs. In the coronal pulp, they are usually spheroidal “pulp stones” (Fig 5-8), interspersed with fronds of so/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


