Chapter 3
Preparing for Definitive Treatment
Aim
To introduce important issues in the assessment of a tooth for definitive root canal treatment and describe preparatory measures including the need for local anaesthesia, occlusal adjustment and simple methods of rubber dam isolation.
Outcome
After studying this chapter, the reader should have a clear view of general and local issues in planning definitive root canal treatment and understand the value of rational preparatory measures including rubber dam isolation.
The immediate management of symptomatic teeth was described in Chapter 2. In subsequent chapters, it will be assumed that acute symptoms have been controlled.
Not Everything That Can Be Root Treated Should Be
Current techniques make it possible to access and root fill just about any tooth, but that does not mean that all damaged teeth should be. Root canal treatment must never be an isolated technical exercise; it is simply a means of preserving teeth for restoration within the context of a holistic treatment plan.
The following questions should be asked:
-
What is the role of the tooth within a broader plan of care?
-
Is it restorable?
-
Can I control infection in it?
-
Are there any additional factors which weigh the case for root canal treatment or extraction?
Decisions should be based on clinical and medical history, clinical examination and recent, good-quality radiographs as well as patient aspirations and finances. Even if large extraoral films have been exposed for general planning, small intraoral films are often justified for greater detail. Images should be projected as near to actual size as possible by the use of a paralleling device (Fig 6-9).
What is the Role of the Tooth Within a Broader Plan?
Questions might include:
-
Is there merit in sacrificing a molar as part of a planned shortened dental arch approach to the mouth?
-
Would preservation of a last standing molar be highly advantageous in avoiding a free-end saddle denture?
-
Would that grossly carious or periodontally compromised canine serve well if the root canal was treated as an overdenture abutment, even if its likely lifespan were limited?
Is the Tooth Restorable?
Patients should not be made promises before teeth have been properly explored and facts are known. Often that is more than just a thorough clinical and radiographic examination (Fig 3-1a).
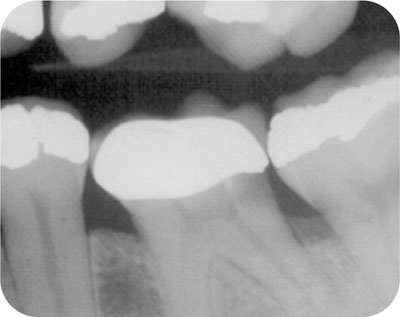
Fig 3-1a Is this tooth restorable? Should the restoration and caries be removed before making any promises?
Defective restorations should be removed and caries ruthlessly excavated, ensuring that the amelodentinal junction is sound at every point, and that the entire crown is fee from soft, infected dentine. Caries is regularly found hiding under radiodense crowns, the only clue being a clinically or radiographically defective margin (Fig 3-2). If there is any doubt, it is better to remove the restoration and caries, discover that the tooth is unrestorable and make alternative plans, rather than fight through infected caries in an effort to preserve a tooth with rubber-like coronal tissue which will fail expensively before long.

Fig 3-2 Removal of this defective crown revealed grossly carious, rubbery coronal tissue.
Teeth with cracks should be examined by transillumination, with stains and wedging devices to ensure that there are no:
-
oblique marginal fractures extending deeply below the alveolar crest and which will be impossible to restore
-
prominent and mobile fractures extending through furcal areas or down the roots of anterior teeth.
Such cases have a compromised prognosis, even with contemporary bonding techniques, and the patient should be made aware of this fact before decisions are made.
If a tooth is unrestorable for any reason, root canal treatment is a waste of time, effort, money, patient confidence and goodwill. It is best avoided from the outset.
Can I Control Infection in It?
Endodontic success is synonymous with the elimination of root canal infection. If a tooth cannot be isolated from the oral flora with a well-fitting rubber dam, is it restorable, and can there be adequate infection control for long-term success?
Canal number, position, calcification and curvature may also present local, technical challenges and raise questions:
-
Can I successfully enter this canal system and eliminate the infection (Fig 3-1b)?
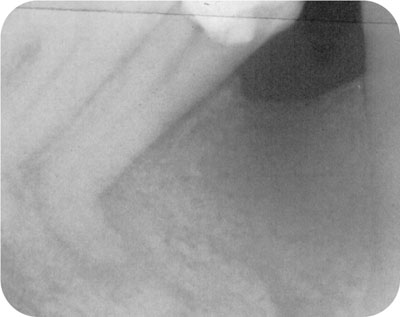
Fig 3-1b Can you really expect to control infection in this tooth?
-
Should I recommend referral or extraction, or should I offer to treat after advising the patient on potential difficulties, and compromise?
Matters may be further complicated in patients with limited opening. Arbitrary measurements of acceptable opening are not helpful; the space n/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


