Chapter 4. Pulp space anatomy and access cavities
A.D.M. Watson
CHAPTER CONTENTS
Summary35
Introduction35
Nomenclature36
Accessory and lateral canals38
Location of apical foramina38
Variations in pulp space anatomy38
Effects of tertiary dentine on pulp space39
Pulp space anatomy and access cavities40
Maxillary central and lateral incisors40
Maxillary canine42
Maxillary first premolar42
Maxillary second premolar42
Maxillary first molar43
Maxillary second molar45
Maxillary third molar45
Mandibular central and lateral incisors46
Mandibular canine47
Mandibular premolars47
Mandibular first molar48
Mandibular second molar48
Mandibular third molar49
Apical closure50
Learning outcomes51
References51
SUMMARY
Knowledge of pulp space anatomy is essential to achieving the objectives of endodontic treatment. The advent of newer imaging techniques including three-dimensional tomography has revealed and confirmed the complex and divergent anatomy of the pulp space. Classical, pre-conceptualized access cavity designs are informative in the understanding of pulp space anatomy. However, they have been replaced by emergent and customized access cavity designs, prepared according to treatment requirements. Unnecessary and excessive destruction of tooth tissue during access cavity preparation remains unwarranted. The wider adoption of magnification and enhanced illumination, especially the clinical use of an operating microscope, is invaluable, greatly aiding access cavity preparation and allowing the detailed examination of the pulp space.
INTRODUCTION
The major factors involved in the development of apical periodontitis are loss of integrity of coronal tooth substance and the entry of microorganisms into the dentine and pulp space. The primary aim of root canal treatment is the removal and exclusion of these microorganisms, their substrates and products from the pulp space and surrounding dentine. Current practice involves the chemomechanical cleaning, followed by the complete sealing of the pulp space. In addition, the need for a good coronal restoration is integral to reducing the risk of pulp space recontamination.
A clear understanding of the anatomy of human teeth is an essential prerequisite to achieving the objectives of adequate access, thorough cleaning, effective disinfection, and complete obturation of the pulp space. Many of the problems encountered during endodontic treatment occur because of the pulp response to irritation and an inadequate understanding of the pulp space anatomy. Both students and clinicians need to familiarize themselves with the intricacies, complexities and aberrations that are likely to occur within the pulp space. The importance of developing a visual picture of the expected locations and numbers of canals in a particular tooth cannot be overemphasized.
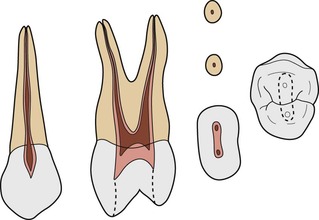
The internal anatomy of human teeth has been studied by many investigators, who have provided a valuable insight into the size, shape and form of the pulp space. Methods of study have included replication techniques, 1,2 ground sections, 3 clearing techniques4.5. and 6. and radiography.7.8.9.10.11. and 12. Clinical radiographs show the forms of roots and pulp canals in two planes only. A third plane exists in a buccolingual direction. The pulp space volume is invariably much greater than the clinical radiograph would suggest. Micro-computed tomography has allowed the appreciation of pulp space anatomy in three-dimensions (Fig. 4.1). More recently, Cone Beam Computed Tomography (CBCT) has increased our knowledge of the pulp space13,14 and allowed the identification of missed anatomy.
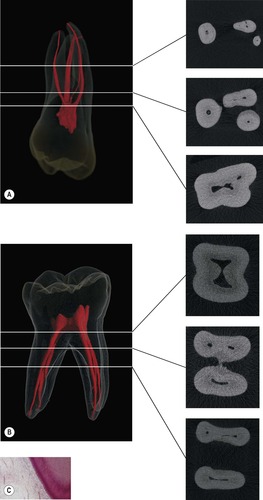 |
| Figure 4.1
Three-dimensional images reconstructed from micro-computed tomography data; cross sections at various levels indicated by corresponding lines. (A) Maxillary molar. (B) Mandibular molar. (C) Cellular arrangement of odontoblast layer.
From Peters 2008, 38 with permission of Quintessence Publishing Co. Ltd.
|
NOMENCLATURE
Anatomically, the dental pulp space is surrounded by dentine to form the pulp-dentine complex. Dentine forms the bulk of the mineralized tissue of the tooth. The dentinal tubules, which are interconnected, make up 20–30% of the total volume of dentine. 15 The number of tubules per square millimetre more than doubles and the area occupied by tubules increases three-fold from the dentine near the amelodentinal junction, to that near the pulp. 16 These differences have a significant clinical effect on the permeability of dentine. It is now realized that the dentinal tubules are an important reservoir of microorganisms when pulpal necrosis occurs. 17 A direct route of contamination from unclean root canals into the periapical tissues may be created by the exposure of infected tubules following root-end resection during apical surgery. 18,19
The pulp space is divided into two parts: the pulp chamber, which is usually described as that portion within the crown; and the pulp canal or root canal, which lies within the confines of the root. The pulp chamber is a single cavity, the dimensions of which vary according to the outline of the crown and the structure of the roots. Thus if the crown has well-developed cusps the pulp chamber projects into well-developed pulp horns. In multirooted teeth the depth of the pulp chamber depends upon the position of the root furcation and may extend beyond the anatomical crown. In young teeth, the outline of the pulp chamber resembles the shape of the exterior of the dentine. With age, the dentinal tubules and the pulp chamber become reduced in size by the laying down of intratubular dentine, secondary dentine and tertiary dentine, particularly in areas where there has been caries, tooth wear and exposure to operative treatment (Fig. 4.2). The pulp chamber may then become irregular in outline. With age, there is also a gradual decrease in pulp space volume, the number of nerves, blood vessels and cells within, but an increase in the fibrous and mineral components. The rate at which the pulps age varies from one tooth to another, and from one patient to another. Calcific changes can lead to the pulp space appearing entirely obliterated radiologically. A residual canal, although radiologically unidentifiable, almost certainly remains within the root as a pathway for microbes to reach the apex and cause periapical changes.
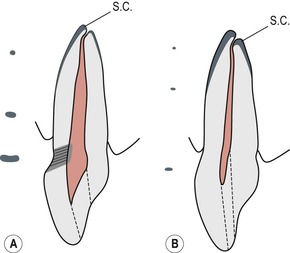 |
| Figure 4.2
Alteration of pulp size with age. (A) Tooth of young adult; large pulp chamber with tertiary dentine under tubules affected by cervical abrasion; small amount of secondary cementum (SC) at apex. (B) Tooth of older patient showing smaller pulp space and greater amounts of secondary cementum that have altered the relationship of the apical constriction to the foramen. Access cavities are indicated by dotted lines. To the left: cross-sections of the root canals are shown at selected levels.
|
The pulp of root canals is continuous with the pulp chamber and normally the greatest diameter is at the pulp chamber level. Because roots tend to taper towards their apex, the canals also have a tapering form which is constricted at the end, the apical constriction, before emerging at the apical foramina, near the root end; rarely do the foramina open at the exact anatomical apex of the tooth. During root development, the pulp and periodontal tissues become separated, maintaining neural and vascular connections through the apical foramina.
The pulp space is complex and root canals may divide and rejoin, and possess forms that are considerably more involved than many textbooks of anatomy have implied. Many roots have additional canals and a variety of canal configurations. Eight separate pulp space configurations have been identified6 (Fig. 4.3). In the simplest form, each root has a single canal and a single apical foramen (Type I). Commonly, however, other canal complexities are present and exit the root as one, two or more apical canals (Types II–VIII).
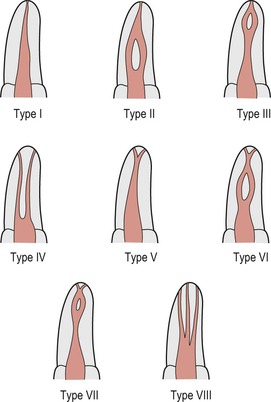 |
| Figure 4.3
Types of canal configuration.
|
Since roots tend to be broader buccolingually than they are mesiodistally, the pulp space is similarly oval in cross-section. The diameter of the root canal decreases towards the apical foramen and reaches its narrowest point 1.0–1.5 mm from the foramen. This point, the apical constriction lies within dentine just prior to the first layers of cementum and is the narrowest point to which the canal tapers. During root development the apical part of the pulp is described as being ‘open’. As the tooth matures, the funnel-shaped foramen closes and constricts to a normal root shape with a small apical foramen. The position of the apical foramen may also be altered, relative to the root apex with the deposition of secondary cementum.
ACCESSORY AND LATERAL CANALS
The pulpal and periodontal tissues not only maintain connection through the apical foramina but also through accessory and lateral canals. A lateral canal can be found anywhere along the length of a root and tends to be at right angles to the main root canal. Accessory canals usually branch off the main root canal somewhere in the apical region. The presence of lateral canals in the furcation areas of molar teeth is well documented and their incidence is relatively high. Patent lateral canals are present in the coronal or middle third of 59% of molars; 20 76% of molars are reported to have openings in the furcation. 21 It has been shown, using a vascular injection technique that these accessory canals often had a greater diameter than the apical foramina, and the blood vessels passing through them often had a greater diameter than those in the apical foramina. 22 The accessory and lateral canals may be demonstrated histologically, by clearing techniques, or clinically on radiographs (Fig. 4.4). The presence of these canals in teeth with necrotic pulps allows microbial toxins to stimulate inflammatory responses in the periapical tissues.
 |
| Figure 4.4
Radiograph of a maxillary central incisor, a lateral canal is revealed after placement of the root filling.
|
LOCATION OF APICAL FORAMINA
The majority of endodontists consider that the apical extent of canal preparation should be determined by the position of the apical constriction in the region of the dentine-cementum junction (Fig. 4.5). Provided that this constriction is not destroyed, the periapical tissues are not damaged during root canal preparation and obturation.
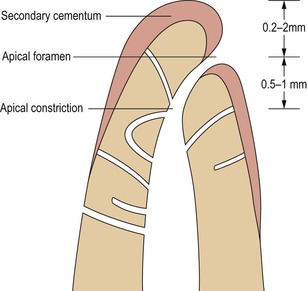 |
| Figure 4.5
Diagrammatic section through apical third of root. The position of the apical foramen varies with age and may be 0.2–2.0 mm from the anatomical apex. The apical constriction may be 0.5–1.0 mm from the foramen.
|
Studies indicate that the apical foramen rarely coincides in position with the anatomical apex. According to various radiological and morphological studies of different teeth,23.24.25.26.27. and 28. the mean distance between the apical foramen and the most apical end of the root is between 0.2 and 2.0 mm. Furthermore, the apical constriction tends to occur about 0.5–1 mm from the apical foramen. 24 Ideally, the apical constriction should be used as a natural ‘stop’ or ‘end point’ in root canal treatment, and the integrity of the constriction should be maintained during treatment if complications are to be avoided. This position can usually be located accurately with an apex locator.29.30. and 31.
VARIATIONS IN PULP SPACE ANATOMY
Variations in tooth form have interested scientists and anthropologists as well as dentists. These studies of variations have primarily been concentrated on the systematic description of dental crown morphology rather than root form. Variations in root form and number are likely to have a direct influence upon the configuration of the root canals in affected teeth. One variation, which has received some attention, is the three-rooted mandibular first molar; surveys of Mongoloid populations indicate a high prevalence.32.33. and 34. The prevalence of other Mongoloid root traits has been less well studied. In clinical practice it is not always possible to observe these variations from radiographs.
In the condition dens invaginatus, the surface of the tooth formed with a deep pit into the pulp space during tooth development, which subsequently becomes a route for infection into the pulp. Depending on the severity of the condition, endodontic treatment will be difficult or very challenging. The most commonly affected tooth is the maxillary lateral incisor. 35,36 In the opposite condition dens evaginatus, the surface of the tooth formed into a very protuberant cusp during tooth development. There is a high risk of this cusp fracturing during function creating a route for infection of the pulp space. The mandibular premolar is most frequently affected and is more often found in Mongoloid people. 37 It is best managed by prophylactic treatment. 38
The descriptions of the frequently occurring root and canal forms of permanent teeth are based largely on studies conducted in Europe and North America, and relate to teeth of predominantly Caucasoid origin. The descriptions may not be wholly applicable to teeth of non-Caucasoid origin. For example, the average lengths of teeth, around which there is wide variation, apply to Caucasoid populations. Practitioners who regularly treat Mongoloid populations are aware that roots are usually shorter. Racial differences and its influence on pulp space anatomy should always be kept in mind.
EFFECTS OF TERTIARY DENTINE ON PULP SPACE
Tertiary dentine is formed by odontoblasts in response to irritation from caries, restorative dentistry or tooth wear. The amount formed is dependent on the degree and duration of irritation. The function of this dentine is to wall off the pulp from the irritants; it is generally of great benefit to operative dentists. However, when root canal treatment becomes indicated, the coronal pulp is then exceedingly small and, therefore, difficult to locate. In addition, canal orifices become narrowed by deposition of tertiary dentine making their identification difficult.
There is no substitute for a good knowledge of pulpal anatomy; however, the clinician should be aided by a good quality preoperative radiograph from which the depth and direction of the root canals can be gauged. When inside the centre of the tooth and attempting to locate the pulp space, illumination and magnification are major assets. Whilst this can be provided by a headlamp and loupes, it is best achieved using an operating microscope. The increased illumination reveals the different colours of circumpulpal and tertiary dentine, so that the access to the root canals can be correctly orientated.
PULP SPACE ANATOMY AND ACCESS CAVITIES
Each line drawing accompanying the description of pulp space anatomy represents, from left to right:
• longitudinal mesiodistal section, viewed from the lingual in anterior teeth and from the buccal in posterior teeth;
• longitudinal buccolingual section viewed from the mesial, and also the axial angulation of the tooth relative to the horizontal occlusal plane;
• horizontal sections through the root(s): (above) 3 mm from apex; (below) at the cervical level;
• incisal or occlusal view.
The classical outline of the access cavity is shown as a dotted line. The size of the pulp cavity shortly after completion of root formation is as shown in pink, and in old age in brown. Line drawings are accompanied, where appropriate, by photographs of cleared specimens to give an insight into the variations of canal form that exist in the adult dentition.
Access cavity design should not be thought of as a one size fits all. Rather they should be developed to suit the specific pulpal anatomy of individual teeth. 39 The classical outline of access cavities is helpful in the appreciation of pulp space anatomy. However, it must be emphasized that rather than pre-conceptualized designs, access cavities should be prepared according to access requirements. Whilst unnecessary and excessive destruction of tooth tissue must be avoided it is important to remember that all caries and the roof of the pulp chamber must be completely removed. If and where necessary, following caries removal, a good temporary restoration should be placed to prevent coronal leakage.
Recently, several authors40,41 have recognized the importance of the systematic development of the pulp space during tooth formation to the understanding of access cavity preparation. This recognition has led to a number of ‘laws’ being postulated, to serve as a guide to clinicians in developing the access cavity and locating accurately root canal orifices (Table 4.1).
| Law of centrality | The floor of the pulp chamber is always located in the centre of the tooth at the level of the cemento-enamel junction (CEJ). |
| Law of concentricity | At the level of the CEJ the shape of the pulp chamber mimics the external anatomy of the tooth. |
| Law of the CEJ | The distance from the external surface of the tooth to the wall of the pulp chamber is the same throughout the circumference of the tooth at the level of the CEJ. The CEJ is the most reliable and consistent feature for ascertaining the position of the pulp chamber. |
| First law of symmetry | With the exception of the maxillary molars, the orifices of the canals are equidistant either side of a line drawn mesial to distal through the floor of the pulp chamber. |
| Second law of symmetry | With the exception of the maxillary molars, the orifices of the canals lie on a line perpendicular to the line drawn mesial to distal through the floor of the pulp chamber. |
| The law of colour change | The dentine of the floor of the pulp chamber is, invariably a darker colour than the roof and walls. With good magnification and illumination this allows the clinician to differentiate and selectively remove tissue. |
| First law of orifice location | The orifices of the root canals are located where the walls and the floor meet. |
| Second law of orifice location | The orifices of the root canals are located at the angles in the floor/wall junctions. |
| Third law of orifice location | The orifices of the root canals are located at the ends of the root developmental fusion lines. |
Maxillary central and lateral incisors
The outlines and pulp cavities of these teeth are similar (Figs 4.6& 4.7). Central incisors are larger with a mean length of 23 mm. Lateral incisors are smaller with a mean length of 21–22 mm. The canal form is usually Type I, and it is extremely rare for these teeth to have more than one root or more than one root canal. Where abnormalities do occur they seem to affect the maxillary lateral incisor, which may present with an extra root, second root canal, dens invaginatus, gemination or fusion. 42,43 The pulp chamber, when viewed labiopalatally, is seen to be pointed towards the incisal and widest at the cervical level. Mesiodistally both pulp chambers follow the general outline of their crowns and are thus widest at their incisal levels. The central incisors of young patients normally have three pulp horns. Lateral incisors usually have two pulp horns, and the incisal outline of the pulp chamber tends to be more rounded than that of central incisors.
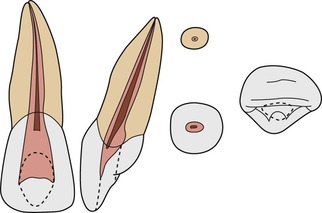 |
| Figure 4.6
Maxillary central incisor with a Type I configuration.
|
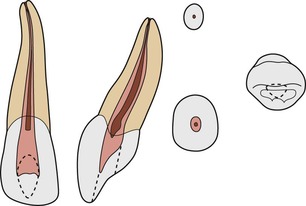 |
| Figure 4.7
Maxillary lateral incisor with a Type I configuration.
|
The root canal differs greatly in outline when viewed mesiodistally and labiopalatally. The former view generally shows a fine straight canal that is seen on a radiograph. Labiopalatally the canal is very much wider and often shows a constriction just apical to the cervix; this view is rarely seen on radiographs and it is important to remember, during treatment, that all canals have this third dimension. The canal is tapered with an oval or irregular cross-section cervically that becomes round only very near the apex. There is generally very little apical curvature in central incisors. The apex of lateral incisors is often curved in a distal/palatal direction. Sometimes the plane in which it lies means the apex is not easily discernible during radiographic canal length determination.
As the teeth age, the anatomy of the pulp space alters with the deposition of secondary dentine. The roof of the pulp chamber recedes, in some cases to the cervical level, and the canal appears very narrow mesiodistally on a radiograph. It is often possible to negotiate a canal that appears very fine or non-existent on a preoperative radiograph. When some incisors are traumatized, their pulps may mineralize, that is, the pulp canal becomes obliterated; subsequent root canal treatment is extremely difficult as mineralization frequently occurs throughout the length of the pulp space.
Access cavities to maxillary incisors
Access cavities in anterior teeth will vary in size and shape according to the dimension of the pulp. They should be designed so that a straight line approach is possible to the apical third of the root without the instruments bending, or binding against the walls of the access cavity or root canal. An access cavity that is too small and close to the cingulum leads to severe stresses in the instrument with binding against the access cavity walls and risks ledge formation apically (Fig. 4.8). The access cavity should extend far enough incisally to allow the instrument to reach the apical part of the canal. Sometimes the incisal edge must be involved if access is to be adequate.
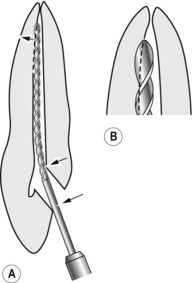 |
| Figure 4.8
(A) The access cavity is too small and close to the cingulum, therefore instruments do not lie passively in the canal and may create a ledge apically. The incorrect access also hinders cleaning of the pulp chamber and near the apex. (B) Enlargement of the apex showing labial ledge and uninstrumented palatal side.
|
As the pulp is broader incisally than it is cervically, the outline should be triangular and must extend far enough mesially and distally to include the pulp horns. Once adequate access has been made into the pulp chamber, the cervical constriction should be removed to facilitate instrumentation of the apical part. The accuracy of initial access is particularly important in the older patient because the pulp space is more difficult to find. It is wise to begin the access cavity close to the incisal edge so that the pulp space can be approached in a straight line.
Maxillary canine
This is the longest tooth, mean length 26.5 mm, and therefore, longer root canal files are often required. It seldom has more than one root canal; the pulp chamber is quite narrow, and as there is only one pulp horn; the pulp is pointed incisally. The general shape of the pulp space is similar to the incisors (Fig. 4.9). The Type I root canal is oval and does not begin to become circular in cross-section until the apical third. The canal is usually straight but may show a distal apical curvature; the curvature depends on the movement of the tooth during eruption.
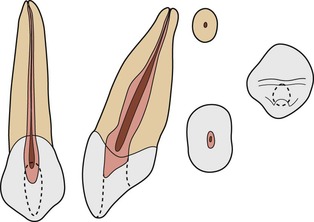 |
| Figure 4.9
Maxillary canine with a Type I configuration.
|
Maxillary first premolar
This tooth generally has two roots with two canals. The frequency of single-rooted maxillary first premolars ranges from 31–39% in Caucasians. 1,44 In people of Mongoloid origin, the frequency of maxillary first premolars with one root is in excess of 60%.45.46. and 47. Three roots have been reported in 6% of cases. 1 A typical Caucasoid specimen has two well-developed fully formed roots that normally begin in the middle third of the roots (Fig. 4.10). The single-rooted condition prevalent in Mongoloid people represents a fusion of two separate roots.
 |
| Figure 4.10
Maxillary first premolar with two roots.
|
Irrespective of origin, this tooth normally has two canals, and in the case of single-rooted specimens these canals may open through a common apical foramen. Many types of canal configuration are to be found in this tooth (Fig. 4.11) and the presence of lateral canals, particularly in the apical region can be as high as 49%. 44 The three-rooted form tends to have three canals, two located buccally and one palatally. Careful study of a preoperative radiograph should help reveal the root canal morphology. However, this morphology may be difficult to visualize radiologically, particularly when the apex is very fine.
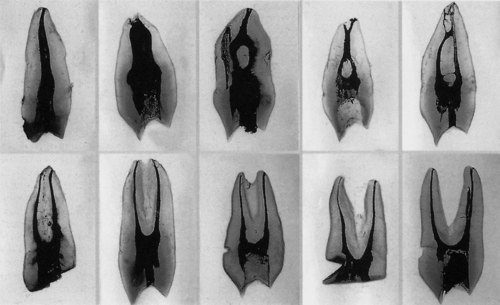 |
| Figure 4.11
Cleared teeth showing various canal configurations in maxillary first premolars.
|
The mean length of first premolars is 21 mm. The pulp chamber is wide buccopalatally with two distinct pulp horns, but is narrow mesiodistally. The floor is rounded with the highest point in the centre and generally just apical to the level of the cervix. The orifices into the root canals are funnel-shaped and lie buccally and palatally under the cusp tip/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


