4
Patient assessment
INTRODUCTION
It is important to take a comprehensive history before undertaking an orthodontic examination. Orthodontic examination should begin as soon as the patient enters the surgery. The general stage of development, including stature/height and the presence of secondary sexual characteristics, should be noted. This information will allow one to determine the amount of growth that may be remaining.
EXTRAORAL ASSESSMENT
Assessment of Skeletal Pattern
The relative position of the maxilla and mandible, termed the skeletal pattern, has a large influence on the relationship of the maxillary and mandibular dentition. The skeletal pattern should be assessed in three dimensions:
- Anteroposterior (AP)
- Vertical
- Transverse.
Anteroposterior Dimension
The aim is to relate the AP position of the mandible to the maxilla and the relationship of these bones to the cranial base. Assessment of the position of each jaw relative to the cranial base gives an indication of which jaw may be contributing to a malocclusion. An assessment of the severity of the discrepancy will help to guide whether treatment can be provided with orthodontics alone or if a combination approach that also involves orthognathic surgery (see Chapter 25) is required. It is important to assess the patient in the natural head position, which is a standardised reproducible head orientation, as the tilt of the head can greatly influence the interpretation of the skeletal pattern. To achieve this, the patient should be sitting upright, relaxed, and looking straight ahead at a distant point at eye level and the teeth should be lightly in occlusion.
The most anterior part of the maxilla and the mandible can be palpated in the midline through the base of the lips (Figure 4.1). The relationship of the mandible relative to the maxilla can be classified as follows:
- Class I – when the mandible lies 2–3 mm posterior to the maxilla (Figure 4.2a). The profile is straight.
- Class II – when the mandible is retrusive relative to the maxilla (Figure 4.2b). The profile is convex. The discrepancy should also be classified as mild, moderate or severe.
- Class III – when the maxilla is retrusive relative to the mandible (Figure 4.2c). The profile is concave. The discrepancy should also be classified as mild, moderate or severe.
Figure 4.1 The anteroposterior relationship of the maxilla to the mandible can be assessed by palpating soft tissue A- and B-points. Ideally A-point should lie 2–3 mm ahead of B-point.
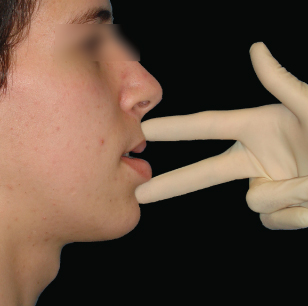
Figure 4.2 Profile photographs showing a (a) Class I, (b) Class II and (c) Class III skeletal pattern.

To determine the position of the mandible and maxilla relative to the cranial base, one imagines a vertical line drawn through soft tissue nasion in the natural head position. This line is termed the zero meridian1,2 and represents the anterior limit of the cranial base. The anterior limit of the base of the upper lip (soft tissue A-point) should lie 2–3 mm ahead and the base of the lower lip (soft tissue B-point) 0–2 mm behind the zero meridian in Caucasians. When making this assessment, it is important to remember that ethnic variation exits in normal lower face protrusion. The face progressively becomes less protrusive as follows: African Caribbean > Asian > whites of northern European ancestry. The term used when both jaws are protrusive is bimaxillary protrusion, which is a common feature in African Caribbeans. As well as using the zero meridian as a guide, other clinical signs which may be present and are suggestive of maxillary retrusion include paranasal flattening, an obtuse nasolabial angle, reduced incisor show at rest, prominent nasolabial folds (due to lack of skeletal support), a flat nasal bridge and lower scleral show.
Vertical Dimension
The vertical skeletal dimension can influence the degree of vertical incisor overlap, lip competency and overall facial aesthetics. There are two methods in which the vertical dimension should be assessed:
- Lower anterior face height (LAFH) proportion
- Frankfort-mandibular planes angle (FMPA).
Vertically in the frontal view, the face can be split into thirds. The LAFH (subnasale-menton) should be approximately equal to the middle face height (glabella-subnasale) for facial balance. However, if the middle face height is of incorrect dimension, the LAFH may be in proportion but also incorrect such that incisor overlap and lip competency are adversely affected. This is why some clinicians additionally measure the absolute LAFH. The normal absolute measurements for LAFH are given in Table 4.1. The LAFH can also be split into thirds and ideally the upper lip should represent one-third of the total height.
Table 4.1 Lower anterior face height measurement in young adults (age 16 years)3
| Male | Female | |
| Caucasian | 72 (6) mm | 66 (4.5) mm |
| African Caribbean | 74 (5.3) mm | 67 (4.8) mm |
Standard deviation is given in parenthesis.
The FMPA is assessed in the profile view and gives an indication of the relationship between the LAFH and posterior face height (i.e. ramus height). It is considered to be normal when the line of the mandibular plane and Frankfort plane intersect in the occipital region. If the point of intersection is anterior to the occiput, the vertical dimension is usually increased and if it lies posterior to the occiput, it is reduced.
Transverse Dimension
The two components of the transverse dimension that should be assessed are:
- Facial symmetry
- Arch width.
It is quite common to find asymmetries in the face, but those that affect the mandible and maxilla are particularly important when planning orthodontic treatment.
The symmetry of facial structures can be assessed by constructing the facial midline between soft tissue nasion and the middle part of the upper lip at the vermillion border. The chin point should be coincident with this line. If there is an asymmetry of the chin point, it is also important to check for a compensatory cant in the maxillary occlusal plane. Asymmetries in the chin point can be produced by a lateral mandibular displacement on closing if there is an occlusal interference.
The relative width of the upper and lower arches affects the transverse relationship of the teeth. Often the maxilla is narrow, which results in a crossbite of the buccal segments if there has been inadequate dentoalveolar compensation (see Chapter 2). On intraoral palpation, the maxilla should be slightly wider than the mandible at the corresponding points. It is important to remember that the absolute transverse dimensions of the maxilla may be normal, but a relative transverse maxillary discrepancy, manifesting as a posterior crossbite, may exist due to incorrect AP positioning of the maxilla/mandible. The AP position can affect the transverse relationship as the dental arches get wider as one moves distally.
As well as the skeletal pattern, the facial soft tissues can influence tooth position. If there is an underlying skeletal discrepancy, the soft tissues may help to guide teeth into a more favourable position (dentoalveolar compensation) so that the occlusal relationship is improved. Soft tissue evaluation should involve examination of the lips, tongue, temporomandibular joints (TMJs) and assessment for habits.
The Lips
The following aspects of the lips should be examined:
- Lip fullness
- Lip tone
- Lower lip line
- Lip competency
- Metho/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


