CHAPTER 4 Limitations in Treating the Edentulous Maxilla
As health care professionals and the general public increasingly understand the benefits of dental implants and accept their use, developing guidelines will allow for predictable treatment outcome for the edentulous patients using fixed, implant-supported prostheses. The use of fixed, implant-supported prostheses in the edentulous mandible has been well studied.1,2 However, the edentulous maxilla warrants special consideration and is the focus of this chapter.
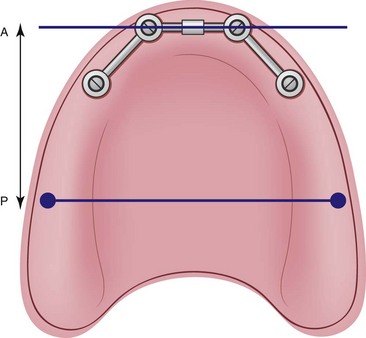
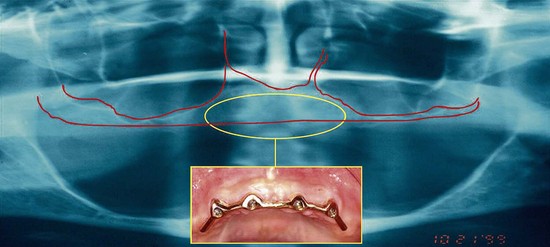
Treatment of the resorbed edentulous maxilla with a fixed profile prosthesis (Figure 4-1), presents with a set of unique problems. Bilateral maxillary sinuses (Figure 4-2) limit the practitioner’s ability to place implants in the posterior portion of the maxilla, which is necessary to establish adequate anterior-posterior distribution (Figure 4-3) of the implants to support the occlusal loads generated and transferred to the alveolus by the fixed prosthesis. Therefore, two to four implants are placed in the premaxilla between edentulous areas 6 through 11 to support the retentive components of an implant-retained, tissue-supported overdenture (Figure 4-4).

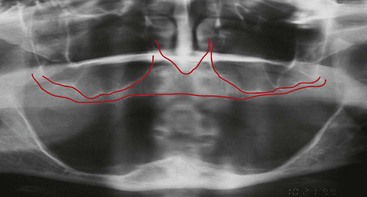
Achieving adequate phonetics and stable masticatory function with a fixed prosthesis are the principle concerns in this group of patients. For the surgeon, the limited residual alveolar bone as well as the existence of the maxillary sinuses pose a number of challenges in treating this group of patients with a fixed prosthesis (Figure 4-5). The comprehensive evaluation of the edentulous maxilla is further complicated by the fact that both bone and soft tissue loss can begin before tooth removal as a result of generalized periodontitis, creating the appearance of long teeth (Figure 4-6). However, some edentulous patients may be missing clinical crowns only, without any accompanying soft or hard tissue loss, which is evident in evaluating the relationship of the cervical portion of the teeth in the clear acrylic copy of their existing full denture against the soft tissues of their edentulous ridge (Figure 4-7). Other patients may be missing a combination of teeth, soft tissue, and bone with associated changes in facial form; in this group, the patients’ denture may be replacing not only their missing teeth, but in many cases the associated soft and hard tissues (Figure 4-8, A and 4-8, B). The dental practitioner must be aware of the extent of tissue loss in the edentulous patient to fabricate an aesthetic and functional fixed prosthesis.





Because of the aforementioned concerns, many patients who are missing their maxillary teeth are often treated with a tissue-supported, implant-retained prostheses (i.e., the maxillary overdenture), or, in many cases, patients are informed that they may not be candidates for implant treatment at all. The further use of a tissue-supported prosthesis, whether a full maxillary denture or a tissue-supported maxillary overdenture, leads to further atrophy of the alveolar bone,3–5 creating a pool of unsatisfied patients who seek alternative treatment options other than the conventional full maxillary denture or the maxillary overdenture.
It is the practice of the author to use physiologic treatment for edentulous patients. The term physiologic treatment refers to the execution of a surgical and prosthetic treatment protocol that biomechanically mimics the same physiologic conditions prior to the removal of the patient’s teeth. The edentulous alveolus undergoes both horizontal and vertical resorption in the absence of internal loading (Figure 4-9). Maintenance of the edentulous alveolar bone is the goal. The existence of the alveolar bone depends largely on the internal loading such as that provided by the tooth roots (Figure 4-10) or dental implants (Figure 4-11).6 Lack of internal loading of the alve/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


