4
Dental Cast Analysis in the Mixed Dentition
Tooth Size–Arch Length Analysis
Why do we need to do a tooth size–arch length analysis in a mixed-dentition patient? Incisor crowding is common in the mixed dentition, because the erupting permanent incisors have larger crowns than the primary incisors [incisor liability] (Moorrees and Chadha 1965). In the posterior segments of the arches, the erupting permanent canines and premolars usually have smaller crowns than the primary canines and molars [leeway space] (Moorrees and Chadha 1965). The main purpose of the mixed dentition space analysis is to differentiate patients with severely crowded arches from those who have up to as much as 4 mm of incisor crowding but who still have enough room in the entire arch, as a result of leeway space, for successful eruption of the permanent premolars and canines and proper alignment of the incisors. The patients just described are excellent candidates for a lower lingual arch or palatal holding arch. Treatment of these patients with a lingual or palatal arch provides them with an important and beneficial service. Intervention with these two preventive appliances can eliminate the need for future orthodontic treatment or simplify future orthodontic treatment.
Patients predicted to have crowding of 5 or more mm in an arch should be referred to the orthodontist. This is also an important service to patients and their parents. Arch length deficiencies occur in the mixed dentition for two reasons: (1) the arch length is too small to accommodate the size of the teeth and (2) arch length is lost because of local causes. When the deficiency results from an imbalance between the size of the teeth and the arch, primary canines are prematurely exfoliated by the erupting incisors and the distances between the distal surfaces of the permanent lateral incisors and mesial surfaces of the primary first molars are small or nonexistent. In crowded dentitions, erupting permanent incisors may erupt outside the line of arch on the lingual and labial sides of the arches. Incisors that erupt too far labially may show recession of the labial gingival tissue.
Local causes that reduce the arch length of a patient include loss of primary teeth through trauma and caries. Caries and restorations that do not restore a carious tooth to its original mesial-distal size contribute to loss of arch length. Ankylosis of a primary second molar can allow the mesial tipping of a permanent first molar, thereby shortening arch length. Permanent canines that erupt ectopically lingual or labial to the line of arch and are impacted are often associated with the loss of arch length.
Prediction of the Widths of Nonerupted Canines and Premolars
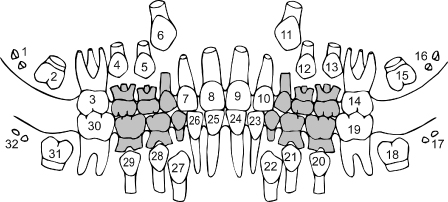
In the early mixed dentition, the permanent incisors and first molars are erupted (Fig. 4.1). The permanent canines and premolars have not erupted. Their mesial-distal widths can be measured on periapical radiographs, but the images are enlarged in comparison to the true widths of the teeth. Orthodontists have devised several methods of predicting the size of the nonerupted canines and premolars. The prediction methods use three basic predictor variables: (1) only erupted teeth, (2) only measurements from radiographs, and (3) a combination of variables 1 and 2. All methods of prediction involve error. The error of a prediction method is called its standard error of estimate. The smaller the standard error of estimate, the more accurate is the prediction method. The lowest standard errors are associated with equations based on multiple regression analysis that used a combination of radiographic and cast predictor variables (Staley and Hoag 1978; Staley, Hu, Hoag, and Shelly, 1983; Staley, Shelly, and Martin 1979). Upper arch multiple regression equations had a range of standard errors from 0.25 mm to 0.4 mm, and lower arch equations had a range from 0.17 mm to 0.28 mm. Multiple regression equations must be calculated for each individual patient and do not have one prediction graph. For convenience, it is more practical to use predictions and graphs based on simple regression analysis.
Figure 4.1. Schema of the early mixed dentition. The primary canines and molars are shaded.
The standard errors of estimate for several prediction methods based on simple regression analysis are listed in Table 4.1. The prediction methods that use the mesial-distal widths of the erupted permanent teeth have the highest standard errors (Moyers 1988; Tanaka and Johnston 1974). The advantage of these methods is that measurements of predictor variables can be taken in the mouth at the time of a clinical examination and do not require periapical radiographs. A complete mixed-dentition space analysis should include a panoramic radiograph.
Table 4.1. Comparison of Standard Errors of Estimate of Several Prediction Methods
| Arch | Prediction Method | Standard Error (mm)* |
| Upper | Iowa, 1984 | 0.48 |
| Upper | Tanaka and Johnston, 1974 | 0.86 |
| Upper | Moyers, 1988 | 1.0 |
| Lower | Revised Hixon-Oldfather, 1980 | 0.44 |
| Lower | Iowa, 1984 | 0.48 |
| Lower | Hixon and Oldfather, 1958 | 0.57 |
| Lower | Tanaka and Johnston, 1974 | 0.85 |
| Lower | Moyers, 1988 | 1.1 |
*Standard error of estimate for one side of the arch.
The Hixon and Oldfather prediction method was based on data from white Americans who participated in the Iowa Facial Growth Study at the University of Iowa. The original prediction method published in 1958 was found to systematically underpredict the size of the canines and premolars (Staley and Kerber 1980). The Hixon-Oldfather prediction method and its revised version are good predictors, because they use the radiographic widths of the patient’s nonerupted premolars, the most efficient predictor variables. The prediction methods that use radiographic images of the nonerupted canines and premolars as predictor variables are more accurate in predicting tooth size in non-Caucasian populations than are prediction methods that use only erupted teeth as predictor variables (Sorbero and Brown-Bryant 2003).
Because the revised Hixon-Oldfather method only predicts the size of lower canines and premolars, a similar method based on data from the Iowa Facial Growth Study was developed for both upper and lower arches (Staley et al. 1984). This method is known as the Iowa Prediction Method. The revised Hixon-Oldfather and Iowa prediction methods have low standard errors of estimate and were successfully validated in a sample of 53 orthodontic patients.
Radiographic Enlargement of Nonerupted Canines and Premolars
We conducted a pilot study to determine image enlargement of an analog periapical radiograph of a lower canine and first premolar in a dry mandible. The radiograph was taken with an 18-inch cylindrical cone angled at +30 degrees at 65 KVP and 10 amperes. The mesiodistal width of the canine was enlarged 7.8% on the radiograph, and the width of the first premolar was enlarged 5.1% (R. N. Staley, 1986, unpublished study). The correction of this enlargement is the primary purpose of the prediction methods described in this chapter. The emerging technology of cone beam computed tomography (CBCT) has reduced image enlargement to about 1% (Pinsky et al. 2006; Williams et al. 2010). CBCT images of nonerupted teeth in mixed-dentition patients will not become frequent in the near future. More likely, clinicians will increasingly take digital periapical images as analog radiography becomes less common. Williams et al. (2010) found similar enlargement of tooth images in digital and analog periapical radiographs. When CBCT images become commonplace, the prediction methods described in this chapter will become obsolete. The CBCT images of the nonerupted canines and premolars can then be directly measured for use in a mixed-dentition space analysis.
Revised Hixon-Oldfather Prediction Method
Records needed to perform the prediction and arch length analysis include (1) periapical radiographs of the unerupted lower premolars taken with a long cone paralleling or right angle technique and (2) a lower study cast. The following steps are taken to complete the prediction of canine and premolar widths and to complete the arch length analysis:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


