CHAPTER 14 Case Presentations
Advanced Procedures
Complete Anodontia
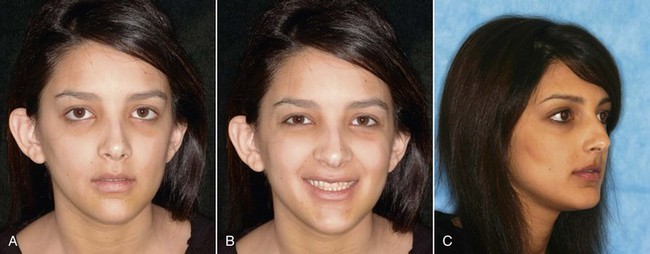
An 18-year-old woman presented with complete anodontia. She had the dentoalveolar development of a 6-year-old in an adult skeleton. The lack of dentoalveolar development resulted in inadequate anterior-posterior (AP) support for the upper and lower lips. The patient had a decreased vertical dimension of occlusion (VDO) and a “wandering” acquired bite consistent with perpetual posturing of her mandible. She had partial primary dentition in her maxillary arch and used a removable prosthesis to replace the missing teeth at positions 8, 9, and 10. She had a full complement of primary mandibular teeth with stainless steel crowns on her anterior mandibular teeth (Figures 14-1 to 14-3).






FIGURE 14-3 Replacement of the missing anterior maxillary teeth with an all-acrylic removable partial denture.
To plan treatment with an implant-supported prosthesis, it was paramount to establish the proper VDO, AP tooth position, and a stable and reproducible occlusion. To accomplish this goal, maxillary and mandibular overdentures were fabricated. Occlusal adjustments were made during the next 4 months to establish a reproducible occlusion (Figures 14-4 to 14-8).

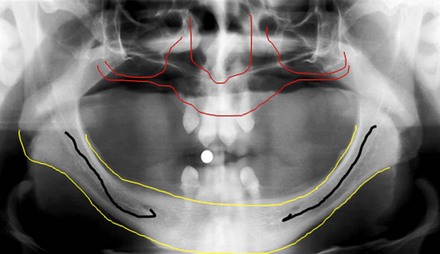
FIGURE 14-4 The patient’s panoramic radiographic examination demonstrates a complete absence of adult dentition.







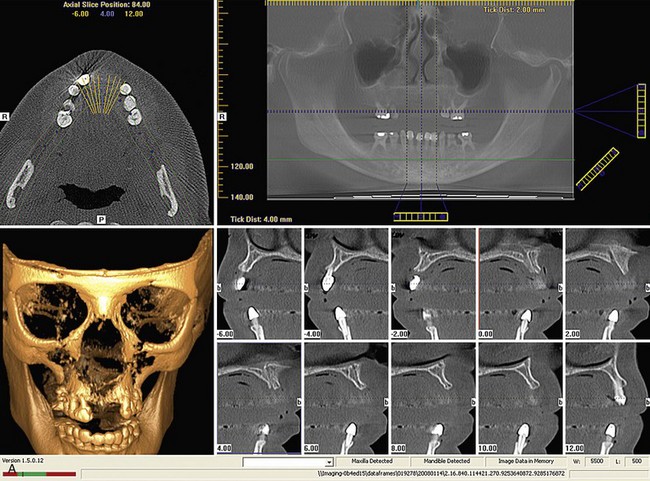
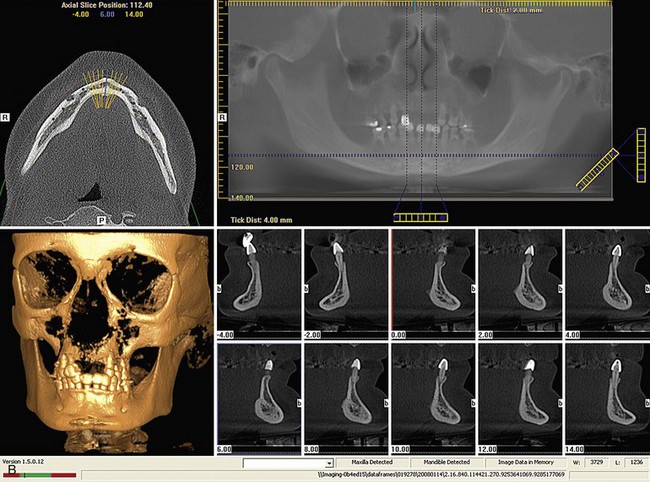
Prior to planning treatment with implants, cone beam radiographic studies of the temporomandibular joints were completed. These studies demonstrated an absence of pathologic conditions in the joint and established a baseline study for comparison with future cone beam radiographic studies of the patient’s joint (Figure 14-9).


FIGURE 14-9 Sagittal and coronal cone beam radiographic studies establish a baseline for future reference.
Systematic pretreatment evaluation of the patient:
















Ectodermal Dysplasia: The Zygoma and Tilted Treatment Concepts
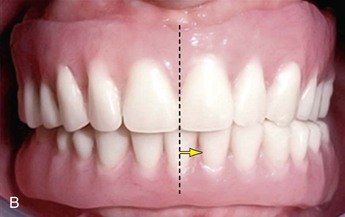
A 24-year-old healthy man presented with ectodermal dysplasia. The facial form indicated collapse of the nasolabial and labiomental angles. In the treatment planning phase, careful consideration must be given to the transition line of the final prosthesis. The intraoral presentation demonstrated partial maxillary and mandibular malformed teeth. A flat maxillary vault and advanced horizontal atrophy of the mandibular residual alveolus were also apparent. The patient maintained maxillary and mandibular removable partial dentures, which were not functional (Figures 14-27 to 14-31).



FIGURE 14-28 Only four anterior maxillary “peg” incisor teeth and two mandibular canines are present.




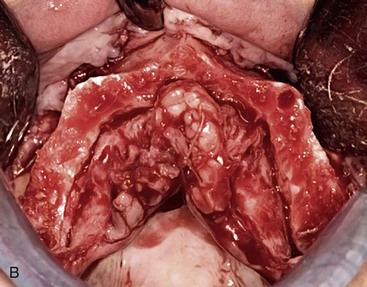
The patient’s panoramic radiographic examination demonstrated a prominent premaxilla and advanced resorption of the posterior maxillary alveolus. The mandible had moderate to advanced resorption in the vertical dimension with retained cuspids only. The presence of zone I bone only indicated that the zygoma treatment concept was appropriate for reconstruction of the maxillary dentition with a fixed profile prosthesis. The tilted implant concept may be considered for treatment of the mandible with a fixed, implant-supported prosthesis (Figure 14-32).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


