Chapter 4
Aesthetic Decisions in Adult Orthodontics
Introduction
With the development of increasingly esthetic orthodontic appliances and shorter treatment times, adults are increasingly seeking orthodontic treatment. With more adults seeking orthodontic treatment and more general dentists providing orthodontic care, there is a need to understand what can be accomplished with adult orthodontics and to clarify the treatment objectives and the treatment planning process.
The availability of esthetic orthodontic treatment modalities and faster treatment means that ignoring orthodontic problems or masking them with restorative dentistry is not as defensible as it may have been in the past. This also accentuates the importance of understanding orthodontic treatment objectives for adult patients.
Esthetic Orthodontic Appliances
Traditionally, orthodontics has required that brackets be bonded to the teeth. While traditionally made of metal, ceramic brackets are clear or translucent and therefore more appealing to adults. An archwire is tied to the brackets with elastics to produce light directional forces needed for tooth movement.
Some brackets hold the wire without ties by way of a locking self-ligating mechanism. Since the elastic ties are prone to discoloration, avoiding the need for elastic ties is an esthetic advantage. Additionally, the self-ligating brackets may reduce friction and thereby reduce treatment time.1
Ceramic brackets, while acceptable to many adults, are still visible. The archwire is usually metal. Translucent fibers may replace the wires and be more esthetic, but they are still not in wide use. There is also the social awkwardness of eating with braces that accumulate food.
Invisalign® (Align Technology Inc., San Jose, CA) appliances overcome many of these problems by being clear and removable. Invisalign is a series of clear removable aligners generated through computer modeling of the treatment objectives. While originally utilized for relatively simple tooth movements, Invisalign is now used for complex orthodontic cases including those involving dental extractions.2
Every system has advantages and disadvantages. There are two challenges with Invisalign. First, it relies on patient use because it is removable. Also, because it is removable, it can lose grip on teeth for certain types of tooth movements. Experienced practitioners successfully match the appliance to the needs of the case and supplement the appliance with auxiliary appliances as needed.
With Invisalign, attachments can give the aligner a better grip on a tooth. These devices are accurately placed tooth-colored bumps that are bonded onto selected teeth and are engaged by the appliance.
Another aesthetic choice of devices to move teeth are lingual braces that are placed on the tongue side of the teeth and are not visible during smiling or speech. New versions of this technique, such as Incognito® (3M Unitek Orthodontic Products, Monrovia, CA), are more accurate and easier for the practitioner to use because the brackets and wires are custom-fabricated for each patient.3 Disadvantages of lingual braces include higher cost and less practitioner experience as compared with conventional braces. In addition, a patient’s tongue must learn to adapt to the brackets on the lingual aspect of the teeth and, potentially, to new speech patterns.
Since patients now have a choice of removable or invisible orthodontic appliances that will fit their lifestyle and new techniques to accelerate therapeutic tooth movements, most adults can find a treatment program that is acceptable to them.
Accelerated Treatment Time
Orthodontic treatment time varies with the difficulty of the case. The average estimated treatment time is 2 years, but in reality, treatment time often 50% greater. This is frustrating for adolescent patients and even more difficult for adults. Fortunately, there are three ways to accelerate this therapeutic interval: increase the accuracy of the orthodontic appliance; enhance the biological response; and use anchor screws to give better anchorage for moving teeth.
Two methods to improve the accuracy of the appliances are OrthoCAD™ (Cadent Inc., Carlstadt, NJ) and SureSmile™ (OraMetrix Inc., Richardson, TX). The former is an indirect bonding technique for more accurate placement of orthodontic brackets. The braces are aligned on a three-dimensional (3D) computer model and then transferred to the patient by means of a positioning tray. SureSmile is a system that allows the orthodontist to perform the treatment virtually on a 3D computer model. These data then drive a robot to bend an orthodontic wire in three dimensions, which will produce the tooth movement designed on the computer model, approximately 34% more rapidly than with traditional techniques.4
The second way of accelerating treatment is to enhance the biological response. Wilckodontics® (Wilckodontics Inc., Erie, PA), also referred to as Accelerated Osteogenic Orthodontics™, is a surgical procedure in which bone surrounding the teeth to be moved is scored and then grafted with bone. These actions stimulate bone to have a major healing response that includes demineralization of the cortical bone.5 The grafting also acts to increase the amount of bone available, improving the range of tooth movement, producing more esthetic and healthier results. This technique routinely allows a conventional 2-year orthodontic treatment to be accomplished in 4–6 months.
A third way of accelerating orthodontics and getting a better result is to use miniscrews, known as temporary anchorage devices (TADs), that are placed into the bone. Whenever a tooth is moved orthodontically, an anchor is needed, and traditionally, other teeth have fulfilled this role. However, the anchor teeth may move unfavorably and time is then lost correcting this unwanted side effect. Also, many times, adequate anchorage is not naturally available, which compromises the treatment result. TADs can help produce tooth movements not previously possible and decrease the overall treatment time.6
Adult Orthodontic Treatment Planning
Assessing each of the three dimensions of the face and dentition is a way to comprehensively evaluate dental and facial esthetics and plan orthodontic treatment goals. In the anterior-posterior dimension, a key orthodontic decision relates to the protrusion or retrusion of the teeth and lips.7 Incisor position is a determinant of lip profile since the lip is influenced by the degree of protrusion or retrusion of the incisors and by the amount of overjet.
In the vertical dimension, orthodontics can affect the amount of vertical display of teeth relative to the lip line. Correction of deep bite or open bite can also change the proportionality of upper and lower facial height. In the transverse dimension, a broader smile can be achieved with expansion.
Midline decisions are another consideration in the transverse plane. These are dental changes that are the focus of this chapter. Although greater changes can be achieved with surgical correction of skeletal structures, oftentimes patients with skeletal disharmonies are treated purely dentally due to cost and/or anxiety issues associated with surgery. Recognition of the limitations of dental treatment as compared with potential surgically produced skeletal changes is an important part of the treatment planning process.8
Anterior-Posterior Objectives
A critical decision in orthodontic treatment planning is where to place the incisors relative to the face and jaws. Incisor protrusion or retrusion can compromise the smile. As previously noted, incisors support the lips and determine lip profile. However, the alteration in lip position relative to incisor retraction or protrusion has considerable individual variability and may be difficult to accurately predict.9
From an esthetic perspective, the position of the teeth should be determined by the upper incisors.10 However, from a practical point of view, lower incisors have less freedom of movement relative to the bone and periodontal support. Therefore, for many orthodontists, lower incisors are pivotal in determining the placement of the teeth within the facial complex.
Incisors are positioned with the thought of balancing the need to reduce crowding, enhancing or maintaining lip profile, improving or maintaining periodontal health, and supporting stability of the result in mind. New approaches, such as accelerated osteogenic orthodontics, help to expand the envelope of bone available for tooth movement, allowing for more consideration of esthetic factors without compromising long-term health or stability.
Once the incisor positioning decision is made, the ideal overjet and overbite will determine the positions of the other teeth. The doctor needs to weigh the influence of both upper and lower incisors since there is no data to support that treatment based on lower incisor position is stabler or has a more predictable esthetic result.11
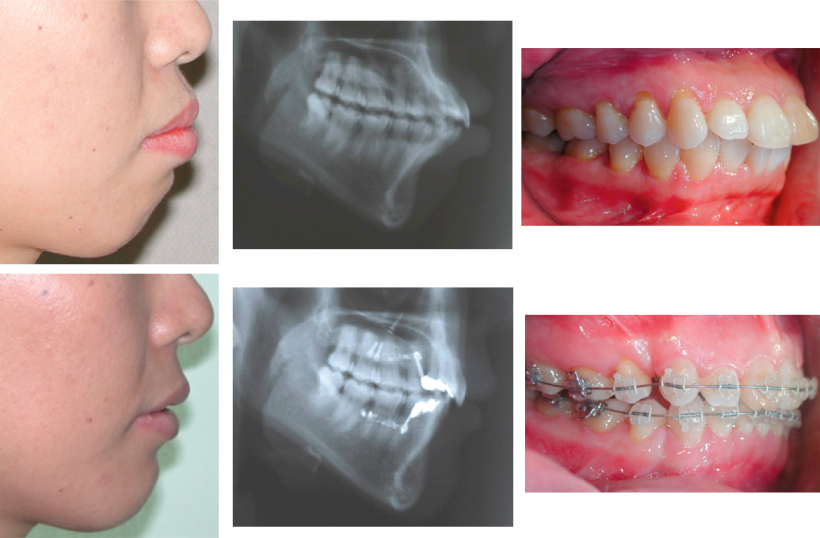
The reduction of lip protrusion as demonstrated in Figure 4.1 clearly corresponds to the retraction of the incisors in this four-bicuspid extraction case.
Figure 4.1 Lip protrusion is reduced by orthodontic retraction of incisors as facilitated by the extraction of four bicuspids.
In adult orthodontics, a compromise in overjet may be defensible if the patient declines surgery and if the upper and lower incisor goals are incompatible with an ideal anterior overjet. In this situation, upper incisors may be placed ideally for esthetics and the lower incisor positioning may be determined by periodontal factors. The patient should be informed that this is compromised treatment and that there are health, function, and stability reasons for achieving an ideal anterior occlusion.
Transverse Objectives
Expansion produces space to help resolve dental crowding and creates a broader smile. Dark corridors may be reduced as demonstrated in Figure 4.2.
Figure 4.2 Orthodontic expansion of arch width creates a broader smile and reduces dark buccal corridors.

Most orthodontists limit expansion in adult orthodontics to as little as possible. Since crowding is very common and doctors and patients prefer nonextraction orthodontic treatment, crowding is often resolved with a combination of modest amounts of expansion, proclination of the dentition, and tooth width reduction. By doing a modest amount of each, crowding can often be resolved without needing to do too much of any one.
Increasing the amount of alveolar bone volume with accelerated osteogenic orthodontic techniques, as noted previously, allows for greater expansion to accomplish esthetic goals, or for more easily creating space without extractions.12
Vertical Objectives
The amount of incisor showing vertically below the upper lip line is an important esthetic factor in orthodontics. The amount of incisor display needs to be evaluated in relation to both the resting lip and th/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


