35
The biology of tooth movement
Table 35.1 Optimal force levels for various tooth movements.
| Tooth movement | Force level (g) |
| Tipping | 30–60 |
| Bodily movement | 60–120 |
| Rotation | 30–60 |
| Extrusion | 30–60 |
| Intrusion | 10–20 |
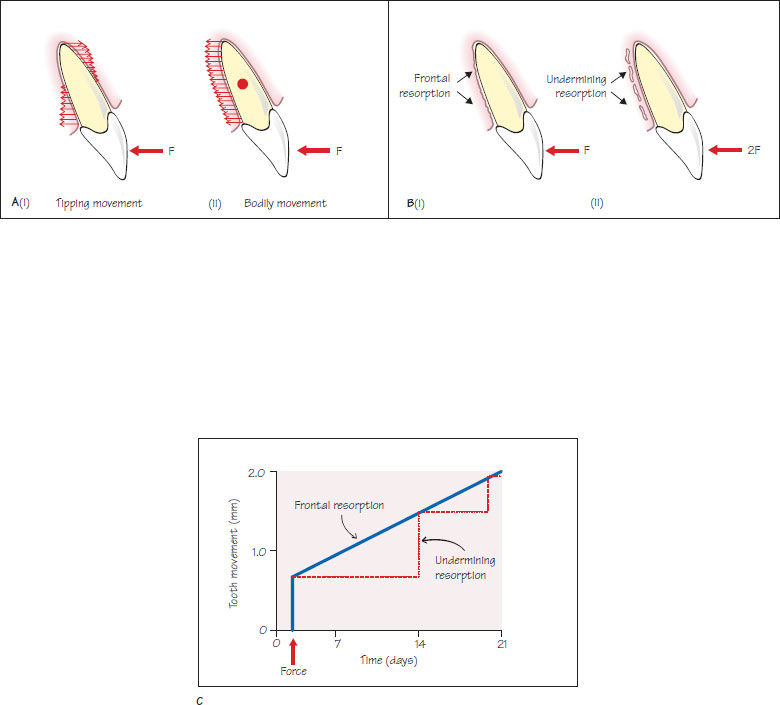
Figure 35.1 (A) (i) Tipping movement results from compressive forces on diagonally opposite ends of the periodontal ligament. These are greatest at the alveolar crest and root apex and reduce to zero adjacent to the centre of resistance. Tension is created in other areas of the periodontal ligament, (ii) Bodily movement results from even compressive forces along one side of the periodontal ligament and tension on the opposite side. (B) (i) Frontal resorption occurs when orthodontic forces do not exceed capillary pressure, (ii) Undermining resorption occurs when capillary pressure is exceeded and hyalinisation occurs within the periodontal ligament. (C) Tooth movement occurring during the application of light (frontal resorption) and heavy (undermining resorption) forces. Undermining resorption results in delayed, large tooth movements because a great thickness of alveolar bone must be removed before the bone that lines the alveolar socket is resorbed. If force levels are maintained this process continues to repeat itself.
The application of a continuous force to a tooth results in remodelling of alveolar bone, reorganisation of the periodontal ligament and tooth movement. Orthodontic tooth movement is a complex process that involves the co-ordinated activity of many cell types and numerous chemical mediators. This chapter provides a summary of the mechanism of orthodontic tooth movement.
Effects of force on the periodontal ligament
The application of a continuous force to a tooth surface results in the development of areas of compression and tension within the periodontal ligament (Figure 35.1A). Tipping forces produce compressive loads that are greatest at the alveolar crest and root apex on diagonally opposite sides. Bodily movement results from even compressive loads along one side of the periodontal ligament.
The magnitude of the force delivered is important in determining the tissue response. Ideally, orthodontic forces should not exceed the capillary pressure within the periodontal ligament as this produces ischemia and tissue necrosis. The optimal force for tooth movement also depends on the type of tooth m/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


