31
Anaesthesia for ENT and maxillofacial surgery
ENT and maxillofacial surgery present unique challenges to the anaesthetist. The proximity of the surgeon to the airway – sometimes in the airway itself – means that the anaesthetist and surgeon share the airway. Thus great cooperation is needed between the two. Access is often restricted due to surgical instruments or drapes. Moreover, the airway itself may be compromised during the operation from pre-existing pathology (tumours/infection) or from blood, bone, etc.; therefore, meticulous assessment and management of the airway is required at all times. Protection of other structures, particularly the eyes, is also important as they may be wrapped in drapes too.
Many different operations are performed but only a few will be discussed here:
- ear: grommets, middle ear surgery;
- nasal: sinus surgery;
- throat: tonsillectomy, laryngsocopy, laryngectomy;
- maxillofacial: orthognathic surgery, free flap;
- emergency surgery: post-tonsillectomy haemorrhage, airway obstruction, trauma.
Preoperative assessment
The patient population comes from diverse groups: mainly children for some ENT procedures (e.g. tonsillectomy and grommets) and elderly patients, often with co-morbidities secondary to tobacco and alcohol, for throat tumours and free flap procedures.
Airway
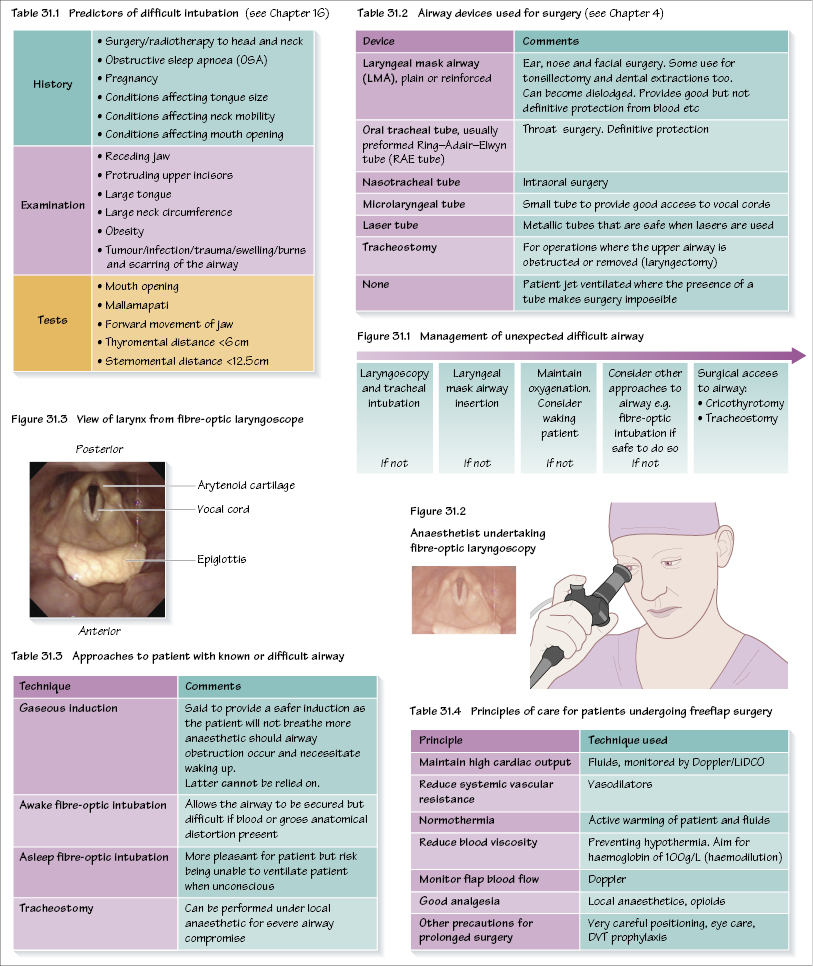
The airway is clearly fundamental to all anaesthetic practice but is pivotal in the management of these patients. The topic is dealt with in Chapter 16, and is summarized in Table 31.1. Of particular importance to ENT patients are:
- A history of obstructive sleep apnoea (OSA), with some patients requiring continuous positive airway pressure (CPAP) at night. These patients may r/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


