Design Criteria for Restorative Dental Materials
As discussed in Chapter 2, restorative materials are exposed to chemical, thermal, and mechanical challenges in the oral environment. The combination of forces, displacements, bacteria, biofilm, fluids, thermal fluctuations, and changing pH contribute to the degradation of natural and synthetic biomaterials. Each patient has a unique combination of these factors. When considering a new or replacement restoration for a patient, the performance history of the patient’s existing restorations can provide insight into the prognosis of the new restoration. The performance of materials in controlled conditions, in vitro and in vivo, is also useful when selecting materials and predicting their service life. Making the final materials choices involves a complex decision-making process that can be informed by principles of product design.
Design Cycle
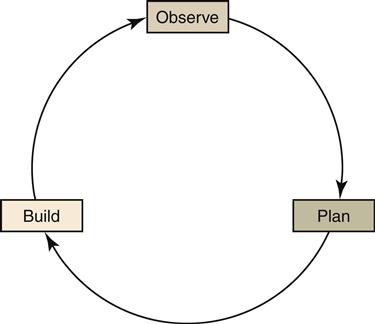
Considering many factors and integrating many specifications into one final product is a requirement of any object that requires fabrication. In product design, a cyclical approach of analyzing and then testing problems is used to determine the best design for the final production piece. Three categories of problem-solving are used in the design cycle: observe, plan, and build. Then the steps are repeated as the time, number of problems, and difficulty of problems allow (Figure 3-1).
To illustrate how this process can be applied to the design of a materials-sensitive product for dental hygiene, we use the simple example of dental floss. The job this product needs to accomplish is removal of interproximal plaque and debris. All interproximal regions and surfaces are not the same. Some interproximal contacts are tight, others are open, and some regions might have proximal restorations with varying degrees of marginal adaptation. The development of a new dental floss product might start with the problem of a potential customer who has a two-surface posterior restoration with an overhang. Current floss products on the market shred or tear when flossing in such a region. This main observation is analyzed and deemed significant, because many people with this problem and similar problems could be helped by a design change to this dental floss. Multiple and varied ideas are generated to address the problem: (1) the dental floss cross section could be a ribbon rather than a rope to ease the floss over the overhang; (2) the floss could be a single strand rather than a braid of multiple strands to reduce the number of surfaces on the floss that could catch; or (3) the floss could be made of a different material or a slippery coating could be added to reduce friction. (Note that all of these designs have been presented to consumers at one time or another.)
Based on these possible design changes, a plan is made that incorporates a method or combination of methods that appear to be most promising in regard to addressing the observed problem. All of the possibilities could have merit, but by selecting those that address the observed problem most directly, one can test the solutions most directly. In this example, we will say that the floss will be formed as a ribbon cross section and a change of material will be made to reduce friction. The new floss is built and tested in simulated and actual environments.
One cycle of our design process for a new dental floss has been completed. We hope to find in our testing that we solved the observed problem. That would be an effective solution. What we may observe through testing our built product, however, is that the material is too slippery to remove plaque effectively, or the ribbon is too wide to stay flat when drawn through the interproximal contact and into the gingival sulcus. Based on these observations, a new plan is made, a new product version is created, and we find that we have completed another design cycle. We repeat this process creating more refined versions of the product that provide more exacting solutions to the observed problems. We also observe use of the product in as broad a range of consumer groups as possible to ensure the product addresses the needs of the target market.
The design cycle for developing new products can be used in the planning of restorations as well. When selecting materials for a restoration, one observes the patient’s oral and medical condition and prioritizes the observed problems. The observation data are integrated with valid materials performance data to create a plan of treatment. A restoration is built and tested for occlusion, compatibility, esthetics, feel, and so forth. Adjustments are made in recurring observe, plan, build steps, refining the restoration to satisfy both patient and clinician.
Evidence Used in Product Design
The entire design cycle is based on evidence. Observation provides evidence about the history of performance of existing materials and solutions and identifies the job that new solutions must perform. The thoroughness of the observation phase depends on the skills and experience of the designer. In the plan phase, material properties and characteristics and test data for performance of materials in controlled conditions are added to the observation data. The build phase integrates knowledge of the job or problem with the skill and experience of the designer and considers variations in the operating conditions and properties and known performance of the materials. Without this systematic and integrative approach, the design process would be haphazard and wasteful. The evidence-based design cycle just described is analogous to evidence-based decision making in health care and evidence-based dentistry.
Evidence-Based Dentistry
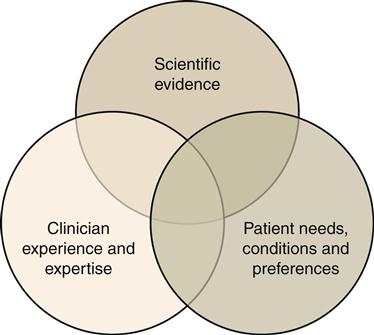
The American Dental Association (ADA) defines evidence-based dentistry as an approach to oral health care that requires the judicious integration of systematic assessments of clinically relevant scientific evidence relating to the patient’s oral and medical condition and history, along with the dentist’s clinical expertise and the patient’s treatment needs and preferences (http://ebd.ada.org). This approach is patient centered and tailored to the patient’s needs and preferences. Our goal is to practice at the intersection of the three circles (Figure 3-2).
Patient Evidence
Patient needs, conditions, and preferences are considered throughout the diagnostic and treatment planning process. Observation of patient needs and medical/dental history occurs first. In this phase, performance of prior and existing restorations, in terms of success or failure, should be noted. This is often a good indicator of conditions in the oral environment and the prognosis of success of similar materials in this environment. The patient’s facial profile and orofacial musculature is a good indicator of potential occlusal forces. Wear patterns on occlusal surfaces are indicators of bruxing, clenching, occlusal forces, and mandibular movements. Cervical abfractions may indicate heavy occlusal contact accompanied by bruxing or occlusal interferences. Erosion on anterior teeth suggests elevated levels of dietary acids, and generalized wear without occlusal trauma could involve a systemic disorder such as gastroesophageal reflux disease (GERD). Any of these conditions would compromise the longevity of restorative therapy. Unusually harsh environments require careful restoration design and selection of materials, sometimes different from the norm.
The options for material to be selected then need to be considered in accord with the problems and needs exhibited by the patient. These data are found in the scientific literature. The integration of patient data and materials data helps make a more fully considered plan for treatment.
Laboratory (In Vitro) Evidence
When searching for scientific evidence, the best available evidence, usually compiled from a review of the scientific literature, provides scientific evidence to inform the clinician and patient. The highest level of validity is chosen to minimize bias. These studies are typically meta-analyses of randomized controlled trials (RCTs), systematic reviews, or individual RCTs. Lower levels of evidence are found in case studies, cohort/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


