28 Diet and Plaque Control
The ingestion of sugars and other highly refined carbohydrates is a necessary condition for dental caries to begin (see Chapter 20). Although mass education to restrict sugar consumption clearly has not worked, restriction of dietary sugars remains an appropriate part of the strategy for controlling caries in a caries-susceptible patient. Development of low- and noncariogenic sugar substitutes also provides a few more options for these patients.
Sugars as a risk factor for dental caries were discussed in Chapter 20. This chapter takes a critical look at the role of dietary approaches to preventing oral disease, at the potential for caries control through the use of sugar substitutes, and at the most appropriate place for oral hygiene in caries control.
NUTRITION AND ORAL DISEASES
Diet refers to the food and drink that pass through the mouth, whereas nutrition is concerned with the absorption and metabolism of nutrients from dietary sources. We stated in Chapter 20 that there is little evidence to show that nutritional deficiencies, either during tooth development or subsequently, cause dental caries. Similarly, in Chapter 21 we discussed how periodontitis cannot be treated as a nutritional disorder. Malnourishment is unusual in the well-fed societies of North America, although it is occasionally seen among some who live in deprived circumstances and among individuals with eating disorders. Where malnutrition is more widespread, as it is in some low-income countries, there is a potential link between malnutrition and the oral diseases, as was discussed in Chapters 20 and 21.
The nutritional status of a patient is rightly the concern of the attending dental professional, and all dentists and hygienists should be sensitive to the signs of nutritional disturbances. When a nutritional disturbance or eating disorder is suspected, referral to a physician or nutritionist is the correct course of action. Even when such a patient is treated successfully for the nutritional problem, improvement in oral status is likely to follow as a consequence only in the most severe cases.
WHAT IS MEANT BY A CARIOGENIC FOOD?
The sugars or other readily fermentable carbohydrates (Box 28-1) in any food can be metabolized by cariogenic bacteria in plaque. Food with this property is termed acidogenic. Acidogenesis is a necessary, though not sufficient, condition for the development of caries. The ubiquity of sugars in processed foods means that a wide range of foods and drinks are acidogenic. Whether an acidogenic food is cariogenic or not will depend greatly on a number of factors specific to the individual who eats it, factors such as predominant bacterial flora, flow rate and buffering capacity of saliva, fluoride availability, and individual immune factors. Whether caries develops or not also depends on how much of the food is eaten and how frequently it is consumed, whether it is eaten in isolation or with other foods, and the nature of any accompanying foods. We therefore cannot be certain whether a particular acidogenic food is cariogenic or not for a particular patient, even if the risk seems high. However, we can be confident about the converse: because acidogenesis is a necessary condition for caries, a nonacidogenic food must also be a noncariogenic food.
BOX 28-1 What Are Cariogenic Foods?
Sugars and other fermentable carbohydrates are part of the etiologic chain in dental caries. The phrase other fermentable carbohydrates is used a lot in the literature, and it sounds both broad and vague. What are these “other fermentable carbohydrates”? The term refers to the cooked or milled starches in the refined flours used in making cookies, biscuits, sweet rolls, croissants, and other processed foods. Their dental significance is that as simple carbohydrates they can be broken down further by the salivary enzyme amylase while still in the mouth and then metabolized by cariogenic bacteria just as sugars are. For that reason these simple carbohydrates are considered potentially cariogenic. Some evidence suggests that starch-sugar mixtures are more cariogenic than sugars alone.19,20,35,71
Starch is a branched or unbranched polysaccharide chain of glucose molecules. The term usually refers to the complex, large-molecule carbohydrates such as those found in potatoes, broccoli, other fruits and vegetables, and whole grains. These are all carbohydrates that have long been viewed as essentially noncariogenic because they break down very little in the oral cavity.60,75 These sugars are part of the structure of fruits, vegetables, and milk, and as such are called intrinsic sugars. Intrinsic sugars are considered virtually noncariogenic when eaten in moderate amounts. Added sugars, sometimes called extrinsic sugars, are held to be the sugars that are metabolized by cariogenic plaque bacteria and trigger the events that lead to demineralization. Some of the literature on this subject expands the term sugars to nonmilk extrinsic sugars.
There is no important difference in cariogenicity between refined sugars and brown sugar. Despite the earlier comment on intrinsic sugars, adherence to a high-fruit diet does not necessarily protect from caries.41 However, as an after-school snack, fruits have considerably more nutritional value than the average candy bar.
The concept of a cariogenic food was too broad to be of practical use in caries control, so attempts were made to determine the cariogenic potential of a food, defined as the food’s ability to foster caries in humans under conditions conducive to caries formation.49 The underlying idea in defining cariogenic potential was to draw up a rank order of cariogenic foods, but a 1986 workshop on food cariogenicity concluded that this approach was unproductive. Although efforts to identify cariogenic foods were not followed up because that category was so broad, the workshop agreed that there was value in identifying nonacidogenic foods, which by definition have no cariogenic potential.30 Such foods can then be confidently recommended to patients who need a sugar-restricted diet.
The cariogenic potential of a single food cannot be satisfactorily tested in human studies because of the “background noise” from other uncontrolled consumption of food components in a normal mixed diet.24 As one example, studies to determine whether the consumption of presweetened breakfast cereals increased caries incidence were unable to control for other crucial variables.26 The 1986 workshop suggested guidelines for testing the cariogenic potential of foods using a combination of several testing regimens, including animal models and in vitro procedures.30 These protocols were intended to identify foods with no cariogenic potential, especially snack foods, but they have not received much attention.
The Swiss government has been testing the cariogenic potential of snack foods since 1982 and has permitted snack foods there to be labeled Zahnfreundlich (which means “tooth-friendly” and implies nonerosiveness as well) if they do not lower the pH of interdental plaque below 5.7 for up to 30 minutes after consumption.48 Under this well-accepted program, tests of food products are carried out telemetrically with a plaque electrode. Accepted products are usually confectionery items sweetened with the sugar alcohols xylitol, sorbitol, mannitol, or maltitol, or with Lycasin, a hydrogenated starch derivative. Fructose does not pass the test.
The impact of this program on the dental health of the Swiss people is difficult to document, however. It is likely to be positive because a high proportion of Swiss children and adults have learned to recognize the “tooth-friendly” logo and to understand that it indicates oral health benefits.74 The concept has spread to a number of other countries, including the United States, where the Food and Drug Administration (FDA) in 1996 permitted the claim “does not promote tooth decay” to be made for sugar-free foods that met specified test conditions.46
SOFT DRINKS
We noted in Chapter 20 that soft drink consumption is associated with caries and that high consumption of soft drinks increases the risk of caries.50 Therefore caries control calls for modest consumption of soft drinks, but in the current social environment it is difficult to promote that message. One obstacle is America’s insatiable thirst for carbonated soft drinks and the nonstop advertising that goes along with it. Even though soft drink consumption has leveled out in the United States over recent years, it averaged 54.2 gallons per person in 2002.18 For years all of this sugar consumption was seen as a matter of no concern, but more recently the high consumption of soft drinks has been linked with the global obesity epidemic,67 an epidemic that is well recognized in the United States. One response to such a problem should be promotion of good nutrition in infancy, but instead the trend in recent years has gone the other way, with juices and soft drinks replacing breast milk, formula, and cow’s milk. This change generally is not beneficial,68 and too many children are already overweight when they begin school. Soft drink companies have been aggressively marketing their products by contracting with cash-poor school districts for the exclusive right to stock the vending machines in the schools, known as “pouring rights.” This, too, is a trend that is not in the public health interest, and it has been vigorously opposed by the American Academy of Pediatrics.4
When we discussed health promotion in Chapter 5 we talked about the necessity for an environment in which people could choose to be healthy. Aggressive marketing of soft drinks, together with what to a child’s eyes is the apparent blessing that school districts give to unrestricted consumption of a particular brand of soft drink, threatens that environment. Health professionals in general agree that soft drinks have little, if any, place in the infant’s diet and should be consumed only moderately in later childhood. This is an issue on which it is logical for dental professionals to join their medical and public health colleagues in promoting healthy diets for children, for clearly both dental and general health concerns are involved.
In view of these issues, it came as a surprise in 2003 when the American Academy of Pediatric Dentistry (AAPD) received a grant from the Coca-Cola Company for research into dental decay.5 Among the concerns raised by this action, the main one is that this alliance will be seen as an endorsement of soft drink consumption in early childhood by the AAPD. This action also puts the AAPD at odds with its medical colleagues in the American Academy of Pediatrics, which has a clear policy of asking schools to reconsider these pouring-rights contracts in the interests of children’s health.4 The AAPD liaison with Coca-Cola also is contrary to the long-standing policy of the American Dental Association to oppose promotion of low-nutrient foods and drinks to children.6
CONSUMPTION OF SUGARS
Consumption of sugars in all forms has continued to rise in the United States for many years. It exceeded 120 pounds (54.5 kg) per capita per year in the 1920s8 and has risen steadily since then. Fig. 28-1 graphs data from the U.S. Department of Agriculture for 1972-2002 to show that, although average consumption of all sugars rose steadily over that period, sucrose consumption declined through 1984 and has leveled out since then. Consumption of monosaccharides continues to increase. Average per capita consumption of all sugars in the United States reached 146.1 pounds (66.4 kg) in 2002, one of the highest levels of national consumption in the world. For contrast, some international values for consumption of sucrose (not necessarily of total sugars) are shown in Fig. 28-2. These data do not include the monosaccharides that account for more than half of consumption in the United States, although monosaccharides are a much smaller fraction of the sugars consumed in other countries.
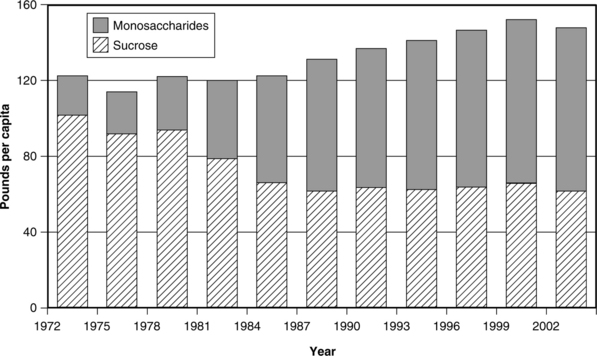
Fig. 28-1 Mean annual consumption of total sugars, sucrose, and high-fructose corn syrup plus other monosaccharides in the United States, 1972-2002.94
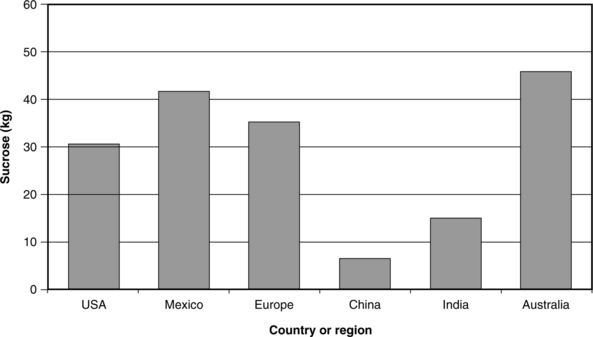
Fig. 28-2 Mean annual consumption of sucrose in the United States, Europe, and four other countries in 1996.
(Data are for sucrose only and do not include consumption of high-fructose corn syrup and other monosaccharides.)93
Most monosaccharide now consumed in the United States is high-fructose corn syrup (HFCS), widely used in place of sucrose in processed foods and soft drinks. HFCS consists mostly of fructose, glucose, and other oligosaccharides. It is used by food manufacturers instead of sucrose because it is cheaper and is produced domestically, so that it is available from a stable market. Corn is a cheap and abundant crop in the United States. But sucrose has such a variety of desirable characteristics from the food manufacturer’s point of view that it is difficult to replace. Not only does it have a sweet taste, but sucrose can be baked and boiled without losing its desirable properties of adding body, luster, and texture to a food product, promoting the emulsification of fats, and acting as a preservative. When HFCS is used instead of sucrose in processed foods, the other desirable qualities of sucrose must come from additives, the use of which arouses anxiety in many people. To complicate the potential health issues, sucrose can be more harmful to human health than was once thought because evidence exists that it contributes directly to the global epidemic of obesity.67
A caveat regarding the data in Figs. 28-1 and 28-2 is that they are all “disappearance” data (i.e., they are derived from the amount of sugar that is produced and then distributed from storage warehouses). Disappearance data do not account for industrial use, wastage, and other losses. Just how much of the “disappeared” sugars actually is consumed by humans is a matter of speculation, but disappearance figures by themselves most likely overestimate human consumption. Still, these data are collected in the same way from year to year, so the trends represented are accurate enough, even if the absolute amounts should not be taken too literally.
In addition to the considerable shift from sucrose to HFCS and other syrups in processed food, two other major changes have taken place in sugar consumption patterns since the early twentieth century28:
CARIOGENICITY OF DIFFERENT SUGARS
Sucrose for years was billed as the “archcriminal” of dental caries because it was considered to be so much more cariogenic than other sugars.72 However, later research has suggested that the differences between sucrose and the various monosaccharides in terms of cariogenic potential are less than originally believed.48,59 This is a difficult issue to study in humans because of the variability of the hu/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


