CHAPTER 27 THE ALL-ON-4 CONCEPT
 Concept of Immediate Function
Concept of Immediate Function
The efficacy of dental implant treatment is well documented in the literature and its further development includes protocols for simplifying the procedures. The Immediate Function protocol is a powerful simplification because it allows the complete rehabilitation to be finalized within the same procedure, maintaining high survival rates in complete edentulous rehabilitations on the long-term follow-up.1–6 Immediate function is considered to be an important psychological factor to the patient and an advantage for the clinical team.7–9
 Clinical Rationale
Clinical Rationale
The All-on-4 concept and its clinical studies were developed and performed in a private clinic, Malo Clinic, in Lisbon, Portugal. The All-on-4 concept is based on the optimal number of four implants for supporting an edentulous jaw with a complete arch prosthesis. The concept benefits from posterior tilting of the two distal implants with a maximum of a two-teeth distal cantilever in the prosthesis (Figure 27-1). The procedures are described elsewhere9,10 and this chapter provides a summary of the protocol, highlighting important details.

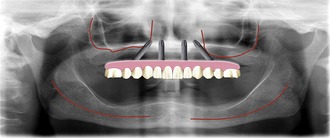
The placement of axial implants in immediate function for complete edentulous rehabilitation has proven to be a predictable rehabilitation procedure in the long term.11–13 However, the loss of posterior teeth, usually at a younger age, leads to the loss of alveolar bone with pneumatization of the maxillary sinus in the maxilla and a more superior position of the mandibular inferior alveolar nerve in the mandible, disabling immediate placement of implants in the posterior regions (Figure 27-2). An alternative could be the use of tilted implants, which allow maximum use of the existing bone with placement of posterior fixed teeth with minimum cantilever, in a region where bone height would not allow the placement of implants (Figure 27-3). The use of tilted implants is fundamental for this rehabilitation concept because it allows the following:

Moreover, finite element analysis leads to the conclusion that there is a biomechanical advantage in using splinted, tilted distal implants rather than axial-oriented implants supporting distal cantilever units when comparing the coronal stress.16
 Inclusion and Exclusion Criteria
Inclusion and Exclusion Criteria
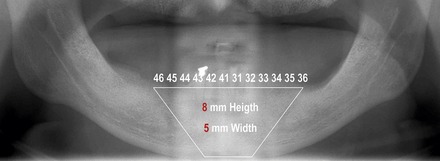
The All-on-4 standard surgical protocol uses two implants placed in the axial position and two posterior implants tilted 45 degrees distally to overcome anatomical limitations. The placement follows the maxillary anterior sinus wall and the anterior loop of the mandibular mental nerve in the mandible. In the mandible, the anatomical inclusion criterion is a bone ridge of at least 4 mm width and ≥8 mm height in the interforamina area (Figure 27-4). The mandibular bone between the canines represents the mandible symphysis, usually present in most edentulous patients. In the edentulous maxilla the anatomical aspects that must be taken into consideration include the location of the anterior wall of the sinus, the crestal width, and the midline. The anatomical inclusion criteria to rehabilitate with an All-on-4 standard technique are a crestal bone ridge of at least 4 mm width and ≥10-mm height from canine to canine.
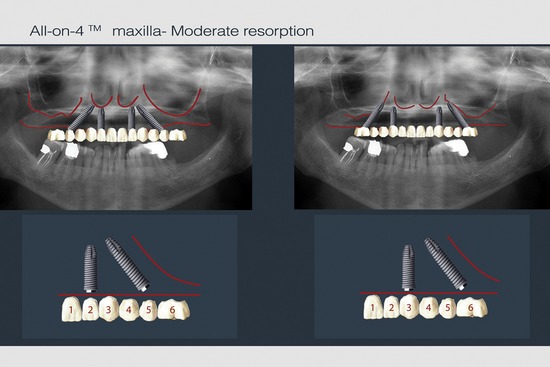
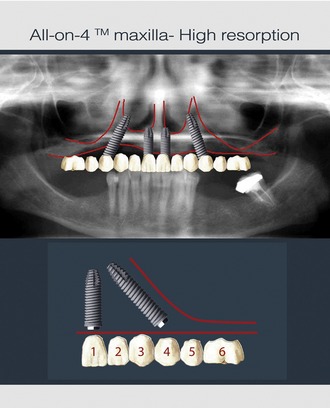
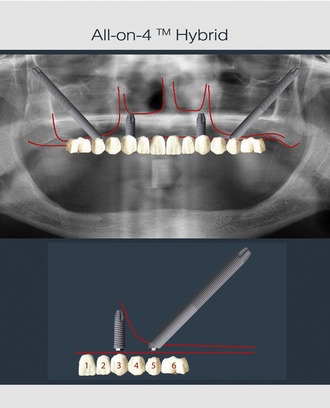
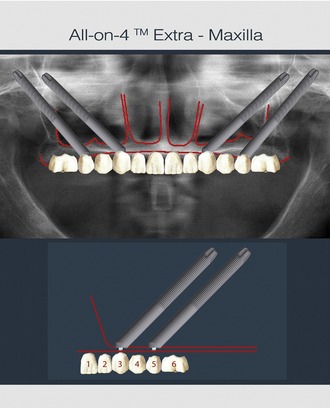
The All-on-4 concept can be used at different degrees of maxillary atrophy because the position of the posterior implant is the determining factor for the interimplant distance. Depending on the degree of resorption, the posterior implant head will emerge at different positions at the ridge crest, usually between the first premolar with advanced resorption (Figure 27-5) and the first molar with moderate resorption (Figure 27-6). If the criteria for the All-on-4 standard protocol are not met, then an All-on-4 hybrid or All-on-4 extra-maxilla procedure should be considered. In the All-on-4 hybrid rehabilitation maxillary anchored implants are used in conjunction with extra-maxillary anchorage implants (anchored in the zygomatic bone) (Figure 27-7), whereas in the All-on-4 extra-maxilla only four extra-maxillary anchorage implants are used (Figure 27-8).
 Advantages
Advantages All-on-4 Standard
All-on-4 Standard
Preoperative photographs and impressions are taken and a careful aesthetic plan is developed according to an Edentulous Rehabilitation Planning Protocol (Table 27-1). With the removable prosthesis in the mouth, two marks are created on the patient’s chin and nose tip using a surgical marker. The distance between these two marks represents the reference point that allows maintaining or increasing the vertical dimension when the immediate prosthesis is placed (Figure 27-9).
TABLE 27-1 Malo clinic edentulous rehabilitation planning protocol
| Checklist | Procedure |
|---|---|
| 1. Vertical dimension (VD) | Willis aesthetic method and Thompson functional method were used in combination (35) for VD determination. Tooth loss is associated with severe bone resorption, which is enhanced by the use of a total removable prosthesis that causes bone and gingival trauma. Bone and tooth losses are responsible for VD decrease. |
| 2. Lip support (LS) | Bone and tooth loss change the orbicularis oris muscle position and create a sagittal intrusion of the upper lip. A wrinkled appearance is a typical observation of the edentulous patient. |
| 3. Smile line (SL) | The future transition zone between natural and artificial gingiva should never be visible. Therefore an evaluation of visible natural gingiva level without the removable prosthesis should be performed to decide if bone reduction is needed during surgery. In the severe atrophic maxillae the natural gingiva usually is not visible with the patient in maximum smile and without the removable prosthesis. This is registered in a digital photograph that is present in the surgical room during surgery. |
| 4. Arch relation | Should be carefully studied before surgery to detect and correct any discrepancy already existing. |
| 5. Occlusion |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


