CHAPTER 25 Growth of the Face and Dental Arches
Historically, patient care in medicine and dentistry has been oriented toward the elimination of disease and the resolution of debilitating conditions. Competent care in dentistry today includes issues related not only to disease and functional disability but also to the patient’s well-being. The appearance of the face and dentition is recognized with increasing frequency as a major factor in human psychosocial health.1
The clinician treating malocclusion is primarily interested in the growth and development of craniofacial tissues as they result in facial and dentoalveolar pattern. Our understanding of how genes express their influence on dentofacial pattern and how environment influences gene expression has advanced at a remarkable pace. How molecular mechanisms are implicated at a clinically relevant level, however, has yet to be elucidated. Mao pointed out that what we understand about induced treatment effects at the macroscopic phenotype level has been described in moderate detail at the cellular level but is only beginning to be described at the level of protein and peptide production.2 For this reason, this chapter discusses dentofacial growth and development at a macroscopic level, from the perspective of the practicing clinician.
THE NATURE OF GROWTH
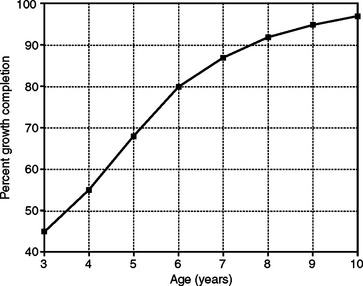
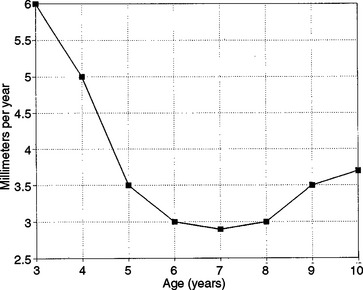
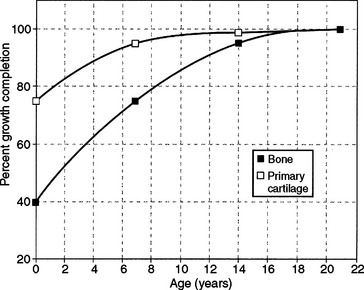
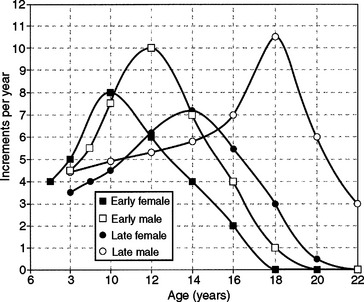
Size increase is typically illustrated in one of two ways. When growth is measured periodically and measurements are plotted as percentages of total growth, the result is a cumulative or distance curve (Fig. 25-1). A human postnatal cumulative curve is characterized by two plateaus and one period of accelerated growth. A second method of graphically demonstrating growth change is by use of an incremental or velocity growth curve (Fig. 25-2). A velocity curve plots growth increments (e.g., centimeters per year) as a function of time. Characteristic of an incremental human growth curve is rapid accelerating prenatal growth, rapid decelerating postnatal growth for the first 2 or 3 years, and a period of relatively slow incremental growth during childhood followed by growth acceleration for 2 or 3 years during pubertal adolescence.
Growth is a complex phenomenon. There is a large volume of information available on craniofacial growth. Moreover, there is little consensus in the literature as to which data or combination of data is most useful to the practitioner committed to making competent decisions about direct patient care. In light of these prevailing circumstances, the following concepts and principles about craniofacial growth are presented in a way that should be clinically useful and difficult to refute. These postulates are derived and adapted in part from widely held tenets about general human growth and development presented by Valadian and Porter.3 The discussion of general craniofacial principles is followed by application of the principles to three areas of craniofacial growth: the face, occlusion, and dental arches. The goal of this chapter is to integrate growth principles in patient appraisal to enhance diagnostic and treatment planning efficacy.
BASIC CONCEPTS OF HUMAN GROWTH
CRANIOFACIAL GROWTH PRINCIPLES
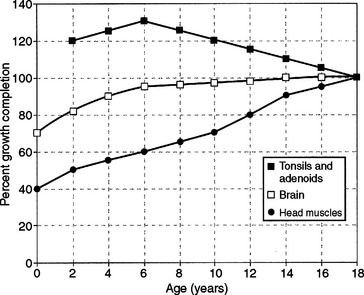
Figure 25-4 Cumulative growth curve for craniofacial neural, muscle, and lymphoid tissues.
(From Linder-Aronson S, Leighton BC. A longitudinal study of the development of the posterior nasopharyngeal wall between 3 and 6 years of age, Eur J Orthod 5:47-58, 1983.)
Growth timing of skeletal tissues also demonstrates variation. Craniofacial bone growth is about 45% completed by birth and 70% completed by 7 years of age. In contrast, primary cartilage of the head and face has achieved approximately 75% of adult size by birth and 95% by 7 years of age (Fig. 25-5). The small amount of primary cartilage remaining in the head and face after middle childhood, however, continues to grow through puberty.
Sperber documents that primary cartilage first appears in the head during the fifth week prenatally.9 By the eighth prenatal week, a cartilaginous mass called the chondrocranium is present and is the precursor to the adult cranial base and nasal and otic structures. By middle childhood, most primary cartilage is replaced by bone in a process called endochondral bone formation.
The overall growth-directing influence of primary cartilage on craniofacial pattern change is most profound in early life. By birth, cartilage comprises a substantial portion of the nasal septum and cranial base. Interstitial expansion of primary cartilage probably has a direct influence on the position of the maxilla by way of the septopremaxillary suspensory ligament, as suggested by Latham10 and later contended by Gange and Johnston.11 The maxilla is most likely thrust downward and forward during infancy and early childhood. The contributions to midface growth of primary cartilage is greatly diminished after middle childhood.
The development of functioning spaces has also received considerable attention as a key concept among craniofacial growth theories.12 The head carries out numerous functions. Some functions are more essential than others, but all require the development and maintenance of spaces. Neural integration is a critical function, and space is required for the brain and central and peripheral nervous system expansion. Respiration and deglutition are also essential to life and require development of nasal, pharyngeal, and oral spaces. Sight, olfaction, hearing, and speech are important but less critical craniofacial functions that also require development of functioning spaces for operation.
According to Moss and Salentijn, a likely craniofacial growth scenario of functioning space development in head and facial patterns includes the following sequence of events.13 Rapid size increase of the brain during prenatal and early postnatal life thrusts the calvarial bony plates outward and the midface forward. Birth invokes a set of functional processes previously not essential for life (i.e., breathing and swallowing). Repositioning of the mandible and tongue takes place to ensure patency of nasal-oral-pharyngeal spaces. The mandible is depressed and thrust forward for these functions to be supported and maintained.
Koski also points out that craniofacial sutures are important growth sites that serve to facilitate calvarial and midface growth.14 Calvarial sutures close by 5 years of age, but some facial sutures remain patent through puberty. Craniofacial bones are thrust apart by primary cartilage and functioning space increases. Sutures enable osseous deposition at bone edges, which allows bones of the face and skull to adapt.
Enlow and Hans have shown that bone, unlike primary cartilage, is subject to environmental controls.16 Bone may assume many forms during growth; it is pressure sensitive, calcified, vascular, and relatively inflexible, and requires a covering membrane for survival. The craniofacial skeleton increases in size by way of surface addition only and increases in shape through differential appositional-resorptive bone growth. This differential growth process accounts for a considerable amount of size increase after middle childhood.
Growth theorists Moss and Salentijn12 believe that the general somatic tissues (i.e., bone, muscle, and connective tissue) demonstrate growth change as a consequence of supporting the functioning operations of the head. Indeed, the research evidence of Linder-Aronson17 and of Harvold and associates18 are convincing in that bone and muscle, as basic tissues, are adaptive and compensatory in nature. Understanding bone and muscle growth may come through understanding the temporal development of functioning spaces and the effects of interstitial cartilage expansion on surrounding tissues.
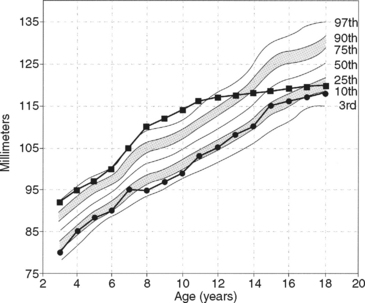
 deviation of several percentile levels during growth, suggestive of abnormalcy.
deviation of several percentile levels during growth, suggestive of abnormalcy.Attributes (craniofacial parts) that are structurally related also maintain a consistent relationship throughout successive stages of growth after infancy. Enlow and Hans16 identify the dental arches of the maxilla and mandible as an example of a structural part-counterpart relationship. An Angle class II skeletal pattern at 3 years of age is maintained into adulthood without corrective therapy. Both dental arches in healthy individuals tend to increase in size at about the same rate. Hence, balanced or equivalent growth tends to maintain architecturally related structures of any craniofacial pattern that is present after 2 years of age.
BASIC CONCEPTS OF CRANIOFACIAL GROWTH
Size increase of the face and calvaria in the three spatial planes is a differential growth process. Scott,19 Meredith,20 and Ranly21 have contributed to an understanding of this process. By birth, the cranial height dimension has attained about 70% of its adult status; cranial width, 65%; and cranial length or depth, 60% (Fig. 25-7). In contrast, only 40% of facial height and 45% of facial length (depth) has been achieved by birth. Face width (i.e., bizygomatic and bigonial), on the other hand, has attained about 60% of adult stature. Growth in face width actually falls between the classic neural and general somatic growth curves.
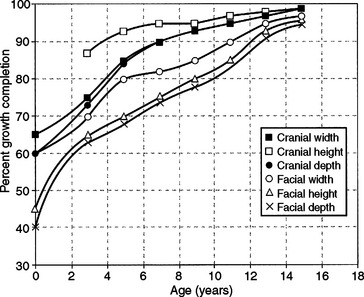
Figure 25-7 Cumulative growth curve for calvaria and face in width, height, and depth.
(From Scott JH. The growth of the human face, Proc R Soc Med 47:5, 1954; Meredith HV. Changes in form of the head and face during childhood, Growth 24:215-264, 1960; Ranly DM. A synopsis of craniofacial growth. New York, 1980, Appleton & Lange.)
After birth, a pattern in facial growth timing emerges. The anterior cranial base completes most of its growth during infancy and early childhood, but frontal and nasal bones continue outward expansion through appositional-resorptive bone growth.22 Growth magnitude and duration are greater for the anterior maxilla than for the forehead but less than for the anterior mandible. The posterior face demonstrates the greatest incremental growth during late puberty.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


