Nutritional and Metabolic Disorders
Nutritional Requirements of Indians
Recommended dietary allowance (RDA) is the amount of selected nutrients considered adequate to meet the known nutrient needs of healthy people. The Canadian equivalent is the recommended nutrient intakes (RNIs). The energy needs of men and women for different activity levels computed on the basis of recommendations made by a Joint Expert Consultation of the World Health Organization (WHO)/Food and Agricultural Organization (FAO)/United Nations University (UNU) in 1985 and by an Expert Committee constituted in 1988 by the Indian Council of Medical Research (ICMR) are as shown in Tables 1 and 2. The ICMR’s RDA is higher than those recommended by the WHO/FAO/UNU.
Table 1
ICMR’s recommended dietary allowance for energy
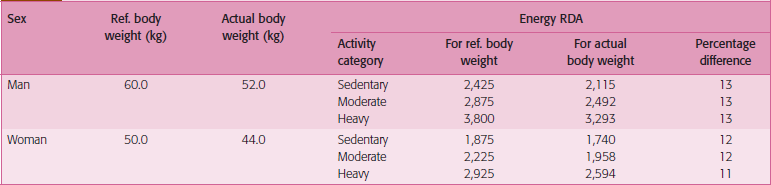
Source: Dr BS Narasinga Rao–Gopalan Oration (2001).
Table 2
Recommended dietary allowance of infants and children
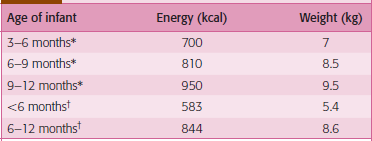
Source: *WHOIFAO/UNO (1985); †ICMR (1988).
Carbohydrates
Functions







Dental considerations
Sugar substitutes have been claimed to be non-cariogenic due to their inability to act as substrates for the enzyme glucosyltransferase. Xylitol is one such commonly used sugar substitute. It has been found to be non-cariogenic. Some studies also show that chewing xylitol gum has cariostatic properties. Other sugar substitutes, sorbitol, aspartame, sucralose have been found to have a negligible effect on the development of caries.
Proteins






Lipids
Dental considerations
1. Some fatty acids, such as oleic acid act as growth factors for lactobacilli, others, such as lauric acids inhibit the growth of streptococci.
2. Long-chain fatty acids may decrease the dissolution of hydroxyapatite by acids.
3. Oral food retention decreases with increased fat intake.
4. Fats may lubricate the tooth and prevent acid penetration into enamel.
5. Fats may produce a film on food particles and prevent partial digestion of food particles in the mouth.
6. Dietary fat delays gastric emptying, enhancing fluoride absorption and increasing tissue fluoride concentration.
Vitamins
Vitamins are classified as fat soluble—vitamins A, D, E, K and water soluble—vitamins B, C.
Vitamin A
Dietary sources
Older literature describes the International Unit of vitamin A. This may be converted to RE as depicted in Table 3:
Table 3
Estimated mean requirement and safe level of intake for vitamin A
| Group | Mean requirement (mg RE/day) | Recommended safe intake (mg RE/day) |
| Infants and children | ||
| 0–6 months | ||
| 7–12 months | 180 | 375 |
| 1–3 years | 190 | 400 |
| 4–6 years | 200 | 400 |
| 7–9 years | 200 | 450 |
| 250 | 500 | |
| Adolescents | ||
| 10–18 years | 330–400 | 600 |
| Adults | ||
| Females | ||
| 19–65 years | 270 | 500 |
| 65+years | 300 | 600 |
| Males | ||
| 19–65 years | 300 | 600 |
| 65+years | 300 | 600 |
| Pregnant women | 370 | 800 |
| Lactating women | 450 | 850 |
Source: Vitamin and mineral requirements in human nutrition, WHO.
Deficiency
Vitamin A deficiency leads to xerophthalmia and night blindness due to degeneration of epithelial cells. Xeroderma can also occur. Mild deficiency may be related to a depressed immune response.
Vitamin D
Sources
The most physiologically relevant and efficient way of acquiring vitamin D is to synthesize it endogenously in the skin from 7-dehydrocholesterol by sunlight (UV) exposure. In most situations, approximately 30 minutes of skin exposure (without sunscreen) of the arms and face to sunlight can provide all the daily vitamin D needs of the body (Table 4).
Table 4
Recommended nutrient intakes (RNIs) for vitamin D
| Group | RNI (mg/day) |
| Infants and children | |
| 0–6 months | 5 |
| 7–12 months | 5 |
| 1–3 years | 5 |
| 4–6 years | 5 |
| 7–9 years | 5 |
| Adolescents | |
| 10–18 years | 5 |
| Adults | |
| 19–50 years | 5 |
| 51–65 years | 10 |
| 65+ years | 15 |
| Pregnant women | 5 |
| Lactating women | 5 |
Source: Vitamin and mineral requirements in human nutrition, WHO.





Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


