23
Deep overbite malocclusion
INTRODUCTION
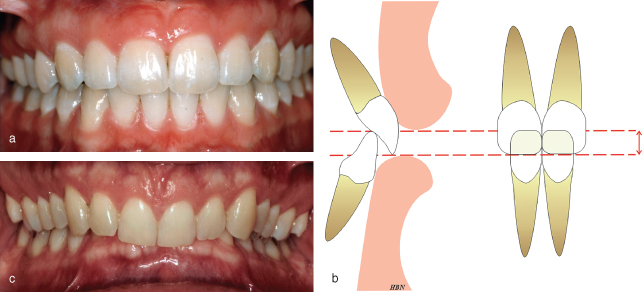
Overbite may be defined as the degree of vertical overlap of the mandibular incisors by the maxillary incisors when the posterior teeth are in occlusion. Overbite depth is usually measured perpendicular to the occlusal plane, either in millimetres or as the amount/percentage of the total crown height of the mandibular incisors that is overlapped by the maxillary incisors. An average overbite occurs when the maxillary incisors overlap the incisal third of the mandibular incisor crowns. In a Class I incisor relationship where the mandibular incisor tips occlude with the cingulum plateau of the maxillary incisors, the overbite depth is 2–4 mm on average (Figure 23.1).
Figure 23.1 (a) A Class I incisor relationship with a normal overbite. (b) The maxillary incisors overlap the incisal third of the mandibular incisor crowns. (c) A deep anterior overbite with the maxillary incisors covering 100% of the mandibular incisor crowns.
Overbite is described in terms of its depth and incisor contact. Therefore, overbite may be:
- Normal
- Reduced (decreased)
- Deep (increased)
and
- Complete to dentition or palatal mucosa
- Incomplete.
In addition, a deep overbite complete to the mucosa palatal to the maxillary incisors, known as an impinging overbite (Figure 23.2a), when combined with poor oral hygiene, may become traumatic, causing irritation and discomfort, and occasionally leading to significant soft tissue damage. In some Class II division 2 malocclusions with minimal overjet the retroclined maxillary incisors may impinge on the gingivae labial to the mandibular incisors (Figure 23.2b). Combined with poor oral hygiene this may lead to traumatic gingival recession.
Figure 23.2 (a) Mandibular incisors impinging on the palatal mucosa. (b) Maxillary incisors impinging on the mandibular labial gingivae.

AETIOLOGY
Anterior deep overbite problems may result either from an upward and forward rotation of the mandible during growth, or from excessive eruption of the incisor teeth, notably the mandibular incisors. Anterior teeth generally erupt until they make contact, either with opposing anterior teeth, palatal mucosa or the resting tongue. The factors that contribute to an anterior deep overbite may be classified as follows:
- Skeletal
- Soft tissue
- Dental.
Skeletal
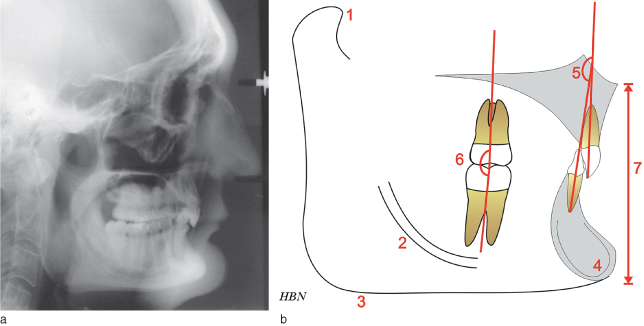
Forward rotation of the mandible, in the direction of mouth closing, is due to increased posterior vertical facial growth compared with anterior vertical facial growth (Figure 23.3a).1 Bjork2 described seven structural signs found on a lateral cephalometric radiograph, which may give an indication to the pattern of mandibular growth. The signs evident in forward growth rotators, which can give rise to an anterior deep overbite are shown in Figure 23.3b.
Figure 23.3 (a) Lateral cephalometric radiograph of a patient with a forward growth rotation of the mandible. (b) Bjork’s seven structural signs indicating a forward mandibular growth rotation. 1: forward inclination of the condylar head; 2: an increased curvature of the inferior alveolar canal; 3: absence of an antegonial notch; 4: forward inclination of the mental symphysis; 5: increased interincisal angle; 6: increased intermolar (and interpremolar) angle; 7: a reduced lower anterior facial height.
Soft tissue
An important aetiological factor in Class II division 2 malocclusion is a high lower lip line, which is thought to guide the maxillary and mandibular incisors to erupt in a more retroclined position. Patients with a reduced lower anterior face height, often described as short face individuals, may have increased mentalis muscle activity. This is sometimes referred to as a strap-like lower lip. Depending on the vertical height of the lower lip, this may cause retroclination of the mandibular incisors, or if a high lower lip position is also present, bimaxillary retroclination of the maxillary and mandibular incisors.
If there is a forward resting tongue position and/or an adaptive tongue to lower lip swallow pattern occurs, the overbite may be deep, but just incomplete to the palatal mucosa.
Dental
Overeruption of the mandibular incisors often accompanies a Class II malocclusion. In Class II division 1 malocclusion with an increased overjet, the mandibular incisors erupt until they contact the palatal mucosa, unless there is a forward resting tongue position and/or an adaptive tongue to lower lip swallow pattern as discussed in the previous section.
In Class II division 2 malocclusion the deep overbite is often the result of retroclination of the incisor teeth. The maxillary incisor cingulum plateau is often poorly defined. The maxillary incisors may also have an increased crown/root angle.
It is important to note that a deep overbite may be partly due to over-erupted maxillary incisor teeth.
INDICATIONS FOR TREATMENT
Anterior deep bite may occur in the primary dentition. If so, it is often associated with a relatively short anterior lower face height, reduced mandibular plane angle and square gonial angles. That is, at this age it is primarily skeletal in nature. If the problem is treated in the primary dentition, it is likely to recur when the active treatment is discontinued. Therefore, at this stage of development, treatment is rarely indicated.
In the early permanent dentition, a deep overbite may need to be reduced if causing trauma to the soft tissues palatal to the maxillary incisors or labial to the mandibular incisors. It is important to note, however, that traumatic overbites are almost always associated with poor oral hygiene. The Index of Orthodontic Treatment Need (IOTN) is currently used in the UK hospital service to prioritise treatment by classifying malocclusions according to treatment need. Only patients with a deep overbite causing palatal or gingival trauma fall into the treatment need category (IOTN 4f).
Deep overbite is often associated with an increased overjet. During orthodontic treatment an increased overjet often cannot be orthodontically corrected until the overbite has been reduced.
METHODS OF OVERBITE REDUCTION
The method most suitable for each patient depends on the treatment objectives, which include the achievement of a stable end result. The dental movements required to reduce a deep anterior overbite may include one or more of the following:
- Relative intrusion of the incisors
- Absolute intrusion of the incisors
- Proclination of the labial segments.
Relative Intrusion of the Incisors
This may be achieved by eruption, extrusion or uprighting (distal tipping) of the premolar and molar teeth. Vertical facial growth is required if the overbite reduction achieved in this way is to remain stable. Molar and premolar extrusion may either be passive (e.g. using an anterior bite plane) or active (e.g. using vertical elastics on fixed appliances).
Absolute Intrusion of the Incisors
This can be difficult to achieve, and requires complex orthodontic mechanics. The mechanics tend to pit incisor intrusion against molar extrusion, thereby inevitably leading to some extrusion of the buccal segments as well as incisor intrusion. The only way to solely achieve true intrusion of incisors is with the use of implants or bone screws (absolute anchorage).
Proclination of the Labial Segments
Overbite depth reduces as the incisor teeth are proclined. A useful two-dimensional geometric model has been described, stating that there is approximately 0.2 mm change in overbite for every degree of incisal angular change e.g. 10° proclination leads to 2 mm reduction in overbite.3 In clinical practice the actual change in overbite depth cannot be accurately predicted by this method alone due to other contributory factors, notably the intrusion or extrusion of the incisors and molars. It must be emphasised that in most cases the pretreatment labiolingual inclination of the incisors must be maintained for stability. Therefore, proclination of the incisors to reduce an overbite may only be used in select cases.
The other option is a combination of orthodontics and orthognathic surgery, in order to reduce a deep overbite surgically.
APPLIANCES AND TECHNIQUES FOR OVERBITE REDUCTION (TABLE 23.1)
Removable Appliances
Anterior Bite-plane
This may be used on a simple upper removable appliance as a preliminary stage of treatment, and is ideally fitted in a growing patient as the permanent dentition is establishing. Clip-over anterior bite-planes (Plint clip) may also be used with upper and lower fixed appliances, giving clearance for placement of lower anterior brackets in Class II division 2 deep bite cases. Overbite reduction occurs by preventing eruption of the mandibular incisor teeth, but allowing eruption of the posterior teeth (Figure 23.4). The lower anterior face height also increases. The addition of cold cure acrylic to the bite-plane allows further reduction of the overbite during treatment. A very useful appliance in a Class II deep bite case is the Ten Hoeve appliance, also known as a ‘Nudger’ (Figure 23.5).4 This appliance, used in combination with headgear, combines the benefits of an anterior bite-plane with distal movement of the upper first molars to aid in Class II correction and bite opening.
Table 23.1 Appliances and techniques for overbite reduction
| Removable appliances | Anterior bite-plane (or clip over bite-plane with fixed appliances) | |
| Dahl appliance (removable) | ||
| Functional appliances | Bite-plane effect, e.g. with activator-type appliances, such as the Medium Opening Activator | |
| Fixed appliances (continuous arch mechanics) | Pre-adjusted edgewise (straight wire) appliance | Continuous heavy flat archwires, e.g. 0.019 × 0.025 inch stainless steel |
| Treating on a non-extraction basis, if possible | ||
| Banding second molars early in treatment | ||
| Placing an increased curve in the upper archwire, and a reverse curve of Spee in the lower archwire | ||
| 0.019 × 0.025 inch preformed counterforce nickel titanium archwires | ||
| Tip-Edge appliance | Anchor bends | |
| Lingual appliances | ||
| Dahl appliance (fixed) | ||
| Fixed appliances (segmented arch mechanics) | Rickett’s utility arch | |
| Burstone’s intrusion arch | ||
| Auxiliaries | Class II intermaxillary elastics | |
| Fixed bite-planes | Turbo props | |
| Composite bite-planes (direct or indirect) | ||
| Headgears | Wedge effect with distal movement | |
| Cervical pull headgear to maxillary first molars | ||
| J-hook headgear to the upper labial segment |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


