Forensic Odontology
 . Personal Identification
. Personal Identification . Dental Identification Procedures
. Dental Identification Procedures . Identification in Disasters
. Identification in Disasters . Identification from Dental DNA
. Identification from Dental DNA . Palatal Rugae in Identification
. Palatal Rugae in Identification . Dental Profiling
. Dental Profiling . The Dentist as an Expert Witness
. The Dentist as an Expert WitnessForensic odontologists delve into:
• Identifying unknown human remains through comparison of postmortem dental evidence with dental records of the presumed deceased.
• Assisting at the scene of a mass disaster and in the victims’ identification.
• Eliciting the ethnicity/population affinity and assisting in building up a picture of lifestyle and diet of skeletal remains at forensic and archeological sites.
• Assessing the sex of skeletonized remains.
• Age estimation of both the living and deceased.
• Analysis and identification of bite marks found on human tissue, animal tissue, and inanimate objects/foodstuffs.
Personal Identification
Traditional methods of identification have included visually recognizing the body, and personal property such as clothing, jewelry and the like. These methods, however, are not very reliable in establishing the identity. Visually identifying a body that is burned or decomposed is not only unreliable but also can be a very traumatic experience for relatives and friends. The more appropriate approach is for forensic experts to analyze physical features present in the body, thus enabling a scientific means to identification.
Dental Identification Procedures
Oral Autopsy
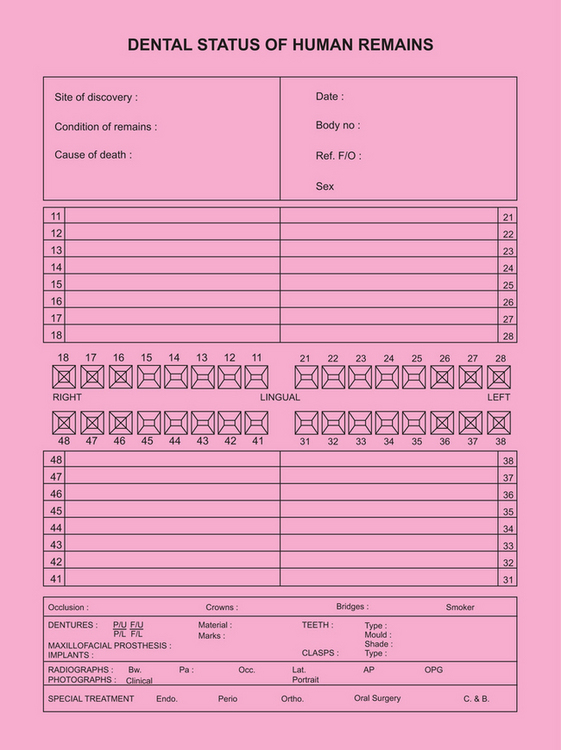
Oral examination is ideally an essential part of the postmortem examination (Fig. 21-1). The forensic dentist who conducts oral autopsy should have adequate knowledge about common postmortem findings such as rigor mortis, livor mortis, decomposition and postmortem artefacts. Rigor mortis may render the jaws rigid and the use of mouth-gags, trismus screws, or intraoral myotomy is essential for jaw separation. In cases of incinerated remains, additional challenges are faced—since teeth may be brittle following exposure to prolonged heat, they need to be reinforced with cyanoacrylate glue prior to examination. According to Griffiths and Bellamy, access for radiography in incinerated bodies can be obtained by removing the tongue and contents of the floor of the mouth in a ‘tunneling’ fashion from beneath the chin. Although oral examination may be challenging at times owing to certain postmortem alterations, the status of each tooth (whether visibly intact, carious/diseased, restored or missing) should be carefully noted. A thorough examination of soft tissue injuries, para-oral hard tissue fractures, and presence of foreign bodies is undertaken and samples of hard and soft tissues may be obtained for further investigations. All information pertaining to the body must be entered into the modified Interpol postmortem dental odontogram (Fig. 21-2).

Figure 21-1 Postmortem dental examination must be thorough and should include a detailed status of the dentition, including whether the teeth are intact, decayed, restored or missing. Reprinted from Nakayama Y et al. Forced oral opening for cadavers with rigor mortis: two approaches for the myotomy on the temporal muscles. Forensic Sci Int 2001;118:37–42, with permission from Elsevier.
Obtaining Dental Records
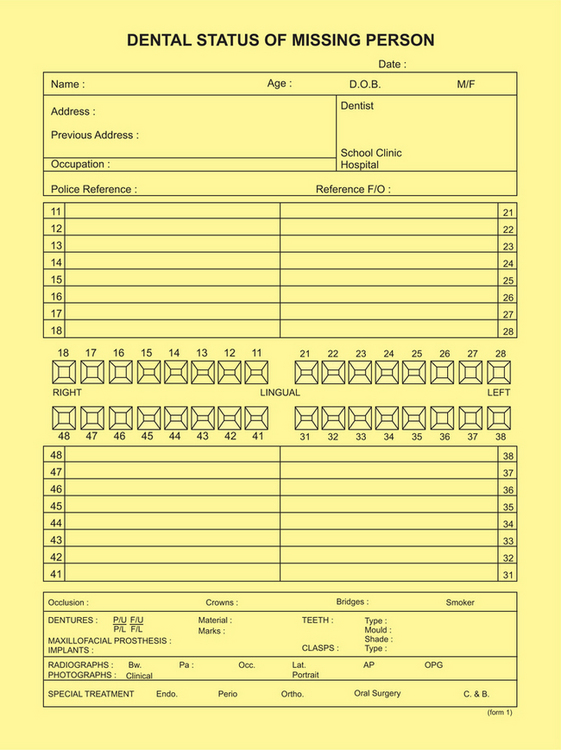
Dental records contain information of treatment undergone and dental status of a person during his/her lifetime, and constitute the antemortem dental data. Dayal and colleagues state that dental records may be obtained from the treating dentist or hospital records. Whenever possible, the original record should be examined. Such records may be in the form of dental charts, radiographs, casts and/or photographs. It is likely that multiple dentists may have treated an individual. Hence, the contents of all available dental records should be transcribed onto the modified Interpol antemortem odontogram (Fig. 21-3).
Comparing Post- and Antemortem Dental Data
Following postmortem examination and transcription of antemortem data, the two odontograms are compared. Features evaluated include tooth morphology and associated bony structures, pathology, and dental restorations (Fig. 21-4). An individual with multiple dental treatment and unusual features has a better likelihood of being identified than someone with no extraordinary dental characteristics. This, however, does not imply that identification relies on extensive dental treatment—comparison should take into account quality rather than quantity. Acharya and Taylor have concluded that a single point of concordance between post- and antemortem data may be sufficient to establish identity, considering, of course, the uniqueness of such a feature and circumstances of the case.
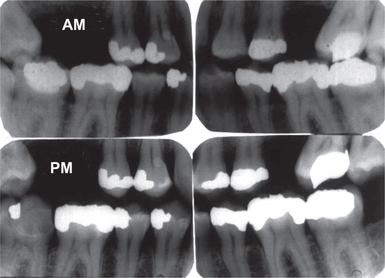
Figure 21-4 Antemortem (AM) and postmortem (PM) bitewing radiographs.
The top two images are bitewing radiographs taken several years prior to death. The bottom two images were exposed on the body with a deliberate attempt to replicate and angulations of the antemortem (AM) images. There are discrepancies between the AM and postmortem (PM) images in terms of number of restorations, but they are explainable on account of the patient having undergone additional treatment in the interval between AM and PM examinations; the discrepancy in tooth 47 (lower right 2nd molar) is due to a dislodged restoration and fractured tooth, possibly due to trauma around the time of death. Reprinted from Wood RE. Forensic aspects of maxillofacial radiology. Forensic Sci Int 2006;159S:S47–S55, with permission from Elsevier.
Writing a Report and Drawing Conclusions
Excludes Identification
The post- and antemortem data are clearly inconsistent. The data contains unexplainable differences which comprehensively indicate a mismatch.
Use of Ameloglyphics in Personal Identification
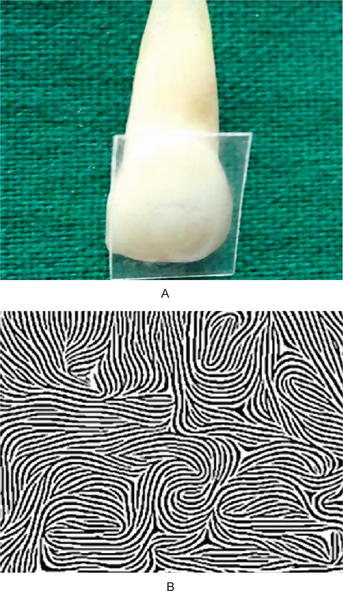
Tooth prints are the pattern formed by the enamel rod ends at the crown surface of the tooth. Manjunath and coworkers recorded the enamel rod end pattern using acetate peel technique (a technique used to study the texture and surface details of rocks and fossils). Based on their recent study that examined 60 subjects and 120 teeth, they have categorized tooth prints into eight different patterns and demonstrated that no two teeth have similar pattern and coined the term ameloglyphics (Fig. 21-5). However they have raised doubts regarding its forensic value since enamel undergoes regressive changes and the course taken by the enamel rods vary at different levels of the enamel.
Identification in Disasters
Dental Section
Forensic dentists are usually part of a team of identification specialists that include anthropologists and fingerprint experts, to name a few. Each team has its own section where postmortem identification is carried out. According to Clark, almost 50% of identifications in disasters are from dental evidence. Therefore, most disaster victim identifications have an odontology section. Representation on this section should be as broad as possible and inclusion of different specialists and dental auxiliaries can be useful. Each team member should be familiar with procedures to be followed in a disaster situation. Information about team activation, the tasks to be performed, and standardized charting methods should be known in advance. Tasks may range from taking radiographs to performing clerical duties. The Interpol’s disaster victim identification guide as well as Vale and Noguchi suggest the division of the odontology section into three sub sections— postmortem unit, antemortem unit and the comparison and identification unit.
Antemortem Unit
Morlang considers the task of the antemortem unit as the most difficult. The members need to collect as much information as possible in the shortest period of time. This begins with locating the dental records of the victims, which requires an extensive network of communication with the police, relatives of the victim and the victim’s dentists. It is essential to re-check the verbal information obtained with the victim’s dentist. This dentist is requested to provide the written records, radiographs and study models to the antemortem unit. The Interpol’s guide has stressed that personnel in this unit should be capable of reading and interpreting all dental records obtained. The quality, quantity, and variety of dental records present a major obstacle to this unit (see Box). Since transcribing and copying could reduce the quality of antemortem information, it is recommended that original records be obtained. All information gathered must be transferred onto the Interpol antemortem odontogram (Fig. 21-3).
Comparison and Identification Unit
A number of computer software programes such as IDENTIFY, ODONTID, CAPMI and IDIS have been developed over the last two and half decades to simplify comparison. In addition, the Interpol has recently facilitated access to and free use of a software program called ‘Plass Data DVI System International’. Using Interpol’s post- and antetmorten forms, the software allows the investigators to enter both post- and antemortem data, which is then analyzed and compared to enhance the matching process and assist in identification. However, these programs merely sort the data, bringing down the number to a few likely post- and antemortem data. Clark stresses that the final identification should always be done by the dentist manually, which is based on personal evaluation of evidence. In problematic cases, it is useful to consult with other methods of identification, such as anthropologists and fingerprint experts. This is reciprocal in nature and adds to the ultimate success of identification in disasters. In fact, the Interpol’s guide states that the success of disaster identification depends on the active participation and cooperation of different identification teams.
Palatal Rugae in Identification
Palatal rugae are ridges on the anterior part of the palatal mucosa on each side of the mid-palatine raphae, behind the incisive papilla (Fig. 21-6). These asymmetric and irregular ridges are well protected by the lips, cheek, tongue, buccal pad of fat and teeth in incidents of fire and high-impact trauma. Furthermore, Muthu, Subramanian and colleagues have found that palatal rugae can also resist decomposition to an extent. Rugae pattern, like teeth, are considered unique to an individual. They seldom change shape with age and reappear after trauma or surgical procedures.
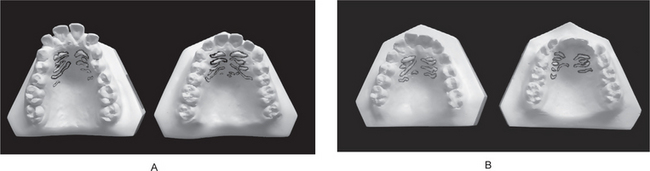
Figure 21-6 Rugae pattern. Courtesy of Dr Dutiganti Santhosh Reddy, Meenakshi Ammal Dental College, Chennai.
Analysis of Rugae Pattern
Thomas and van Wyk have manually traced rugae patterns from post- and antetmortem dentures on to clear acetate (transparent plastic sheets) and then superimposed these tracings on photographs of plaster models. More recently, Limson and Julian have developed a computer software program which makes use of the principle commonly employed in fingerprint analysis. The method used digitized images of the palate on which characteristic points were plotted on the medial and lateral extremities of all rugae (Fig. 21-7). The plotted points were assessed by the software program and the information stored sequentially, corresponding to the pixel position. These researchers obtained up to 97% accuracy in identifying individuals in a simulated post- and antemortem comparison of the palatal rugae. Significantly, in their analyses, the authors have bypassed any form of classification suggested previously. In fact, Thomas and Kotze state that, considering the complex nature of rugae patterns, a universally acceptable classification may not be feasible and, as long as the technique used to compare the rugae is accurate, one need not conform to a particular classification.
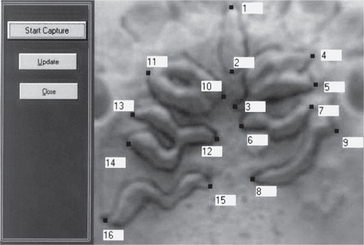
Figure 21-7 Points plotted manually on the image of palatal rugae. Reprinted from Limson KS and Julian R. Computerized recording of the palatal rugae pattern and an evaluation of its application in forensic identification. J Forensic Odontostomatol 2004;22(1):1–4, with permission of author and journal.
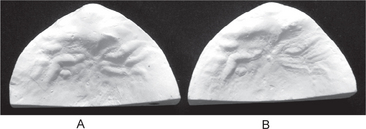
Furthermore, a recent study by Ohtani and coworkers suggests that high accuracy rates in postmortem identification from palatal rugae can be obtained using straightforward visual comparison of post- and antemortem rugae patterns obtained from dentures (Fig. 21-8), and neither a classification protocol nor computeraided method is mandated. These authors did, however, infer that more complex the rugae pattern, greater the tendency for non-identification.
Dental Profiling
Identifying Ethnic Origin From Teeth
Non-metric Dental Traits
Winging
This is an indirect crown trait. It is characterised by the bilateral labial rotation of the distal margins of maxillary central incisors. The incisal edge of the central incisors, taken together, appears ‘V’ shaped from the occlusal aspect. Winging was observed in 16% of the Indian population.
Mandibular Molar Groove Pattern
• When the mesiolingual and distobuccal cusps are in contact, the resultant groove pattern is referred to as the Y-groove.
• When the mesiobuccal and distolingual cusps are in contact at the central fossa, the groove pattern is known as the X-groove.
• When all major cusps are in contact at the central fossa, the groove pattern takes the form of a ‘+’ sign.
Four-cusped Mandibular Molars
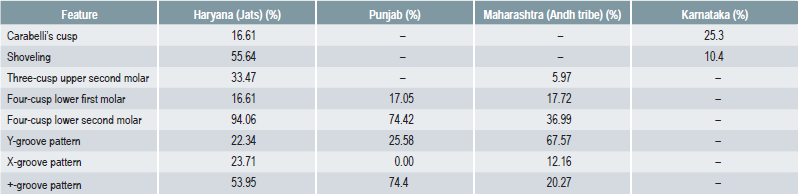
Table 21.1 reveals differences between populations from various regions of India for some of the features described above. Dissimilarities exist between different regions of the world, particularly between the major subdivisions of humankind, namely Eurasians, Africans, East Asians, and Native Americans. The range of dental variation among humans, however, is so great that several non-metric traits must be considered together before concluding on ethnic or population origin. Of the preceding features, some have aroused great interest owing to their high frequency in certain populations, while the occurrence of others is uncommon and, in some instances, rare. One must bear in mind that the high and low incidence of a non-metric trait is equally important in identifying a particular population/ethnic group. For example, people of European, West- and South-Asian origin (Eurasians) may exhibit four-cusped lower first molar, Carabelli’s cusp and three-cusped upper second molar in relatively high frequency, but features such as shoveling and Y-groove pattern do not occur often among them. On the other hand, four-cusped lower second molar is infrequent while shoveling and three-cusped upper second molar is commonly seen among East Asians. One is advised to remember, however, that the frequency of occurrence of many non-metric traits overlap in different population groups. Therefore, the use of such morphological characters for identification should be used carefully and judiciously.
Sex Differentiation
Sexing from Craniofacial Morphology and Dimensions
The use of morphological features of the skull and mandible (Table 21.2) is a common approach used by anthropologists in sexing. A number of features are known to show variation between the sexes. However Botha and Chandra Sekharan, in separate studies, caution that most of these features are not reliable until well after puberty. Even then, no single feature is characteristic and the use of multiple features tends to be more accurate. Williams and Rogers found that sex could be predicted correctly in 96% of cases using different features of the skull and mandible. Furthermore, they observed that using a constellation of just six traits—mastoid process, supraorbital ridge, size and architecture of skull, extension of the zygomatic arch beyond the external auditory canal, nasal aperture and gonial angle (on the mandible)—the accuracy of sex determination was 94%. This indicates that craniofacial morphology can be used to determine sex of skeletal specimens with a high degree of precision. While some authors believe that skull traits are affected by changes in old age, Williams and Rogers found no such effect.
Table 21-2
Craniofacial morphologic indicators of sex
| Skull features | Male | Female |
| Size/architecture | Big/rugged | Small/smooth |
| Frontal and parietal eminence | Small | Large |
| Forehead | Sloping |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


