20 PONTIC DESIGN
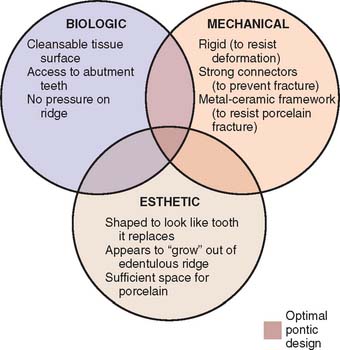
Pontics are the artificial teeth of a partial fixed dental prosthesis (FDP) that replace missing natural teeth, restoring function and appearance (Fig. 20-1). They must be compatible with continued oral health and comfort. The edentulous areas where a fixed prosthesis is to be provided may be overlooked during the treatment planning phase. Unfortunately, any deficiency or potential problem that may arise during the fabrication of a pontic is often identified only after the teeth have been prepared or even when the definitive cast is ready to be sent to the laboratory. Proper preparation includes a careful analysis of the definitive dimensions of the edentulous areas: mesiodistal width, occlusocervical distance, buccolingual dimension and location of the residual ridge. To design a pontic that meets hygienic requirements and prevents irritation of the residual ridge, particular attention must be given to the form and shape of the gingival surface. Merely replicating the form of the missing tooth or teeth is not enough. The pontic must be carefully designed and fabricated not only to facilitate plaque control of the tissue surface and around the adjacent abutment teeth but also to adjust to the existing occlusal conditions. In addition to these biologic considerations, pontic design must incorporate mechanical principles for strength and longevity, as well as esthetic principles for satisfactory appearance of the replacement teeth (Fig. 20-2).
The pontic, as it mechanically unifies the abutment teeth and covers a portion of the residual ridge, assumes a dynamic role as a component of the prosthesis and cannot be considered a lifeless insert of gold, porcelain, or acrylic.1
PRETREATMENT ASSESSMENT
Certain procedures enhance the success of an FDP. In the treatment-planning phase, diagnostic casts and waxing procedures may prove especially valuable for determining optimal pontic design (see Chapters 2 and 3).
Pontic Space
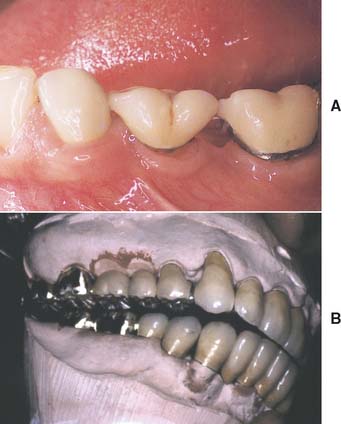
One function of an FDP is to prevent tilting or drifting of the adjacent teeth into the edentulous space. If such movement has already occurred, the space available for the pontic may be reduced and its fabrication complicated. At this point, creating an acceptable appearance without orthodontic repositioning of the abutment teeth is often impossible, particularly if esthetic appearance is important. (Modification of abutments with complete-coverage retainers is sometimes feasible.) Careful diagnostic waxing procedures help determine the most appropriate treatment (see Chapters 2 and 3). Even with a lesser esthetic requirement, as for posterior teeth, overly small pontics are unacceptable because they trap food and are difficult to clean. When orthodontic repositioning is not possible, increasing the proximal contours of adjacent teeth may be better than making an FDP with undersized pontics (Fig. 20-3). If there is no functional or esthetic deficit, the space can be maintained without prosthodontic intervention.
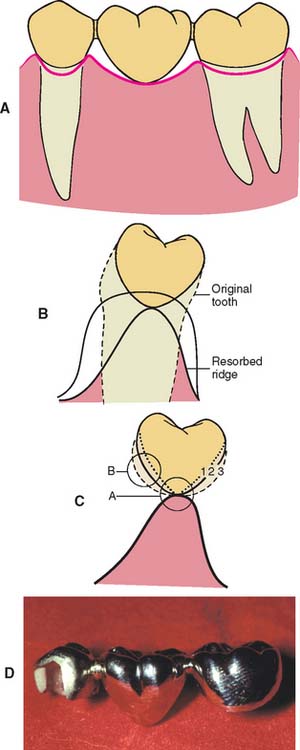
Residual Ridge Contour
The edentulous ridge’s contour and topography should be carefully evaluated during the treatment planning phase. An ideally shaped ridge has a smooth, regular surface of attached gingiva, which facilitates maintenance of a plaque-free environment. Its height and width should allow placement of a pontic that appears to emerge from the ridge and mimics the appearance of the neighboring teeth. Facially, it must be free of frenum attachment and be of adequate facial height to sustain the appearance of interdental papillae.
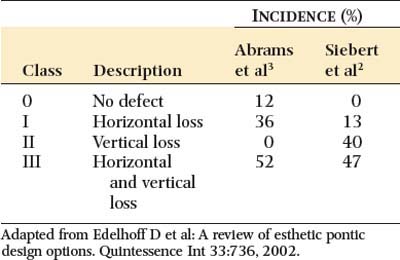
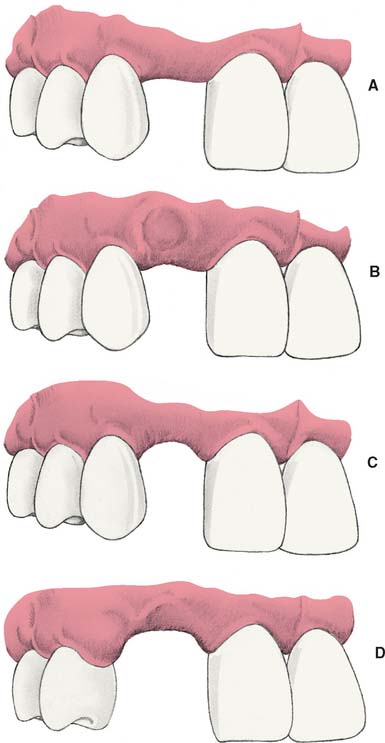
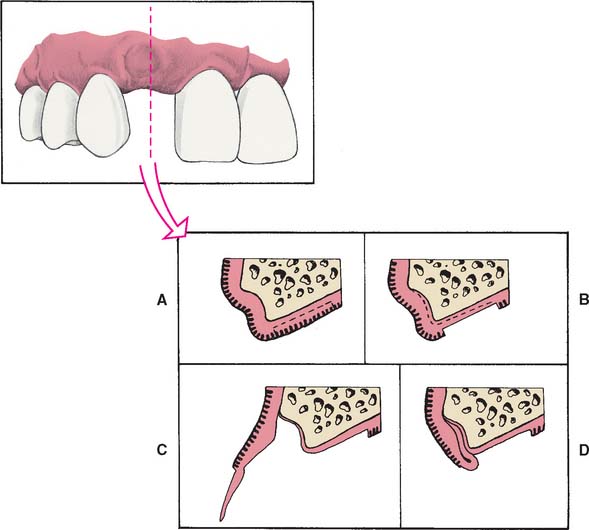
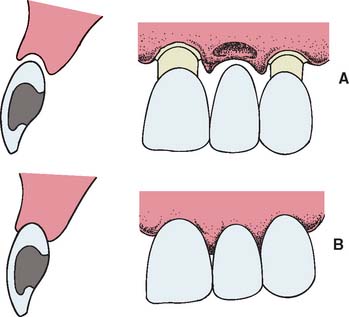
Loss of residual ridge contour may lead to unesthetic open gingival embrasures (“black triangles”) (Fig. 20-4A), food impaction (Fig. 20-4B), and percolation of saliva during speech. Siebert2 classified residual ridge deformities into three categories (Table 20-1 and Fig. 20-5):
There is a high incidence (91%) of residual ridge deformity after anterior tooth loss3; the majority of these are Class III defects. Because patients with Class II and III defects are frequently dissatisfied with the esthetics of their FDPs,4 preprosthetic surgery to augment such residual ridges should be carefully considered.

Surgical Modification
Although residual ridge width may be augmented with hard tissue grafts, this is usually not indicated unless the edentulous site is to receive an implant (see Chapter 13).
Class I defects
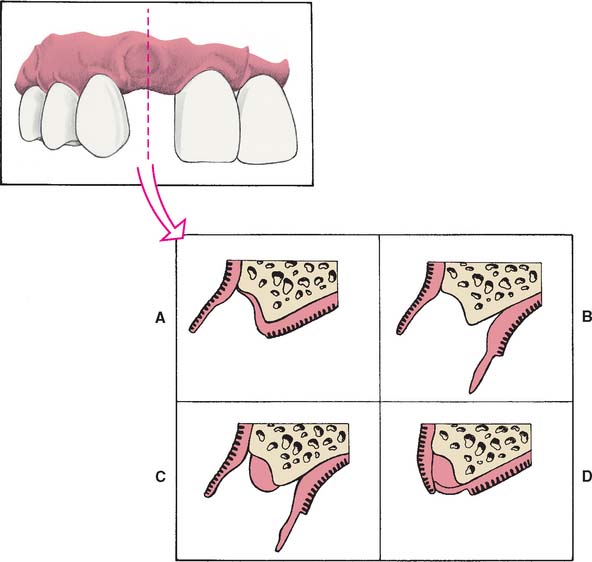
Soft tissue procedures have been advocated for improving the width of a Class I defect; however, because Class I defects are infrequent and are not esthetically challenging, surgical augmentation of ridge width is uncommon. Paying careful attention to interim pontic contour helps the operator identify patients who would benefit from surgery. In the roll5 technique, soft tissue from the lingual side of the edentulous site is used. The epithelium is removed, and the tissue is thinned and rolled back upon itself, thereby thickening the facial aspect of the residual ridge (Fig. 20-6). Pouches may also be prepared in the facial aspect of the residual ridge6 into which subepithelial7,8 or submucosal9 grafts harvested from the palate or tuberosity may be inserted (Fig. 20-7).
Class II and III defects
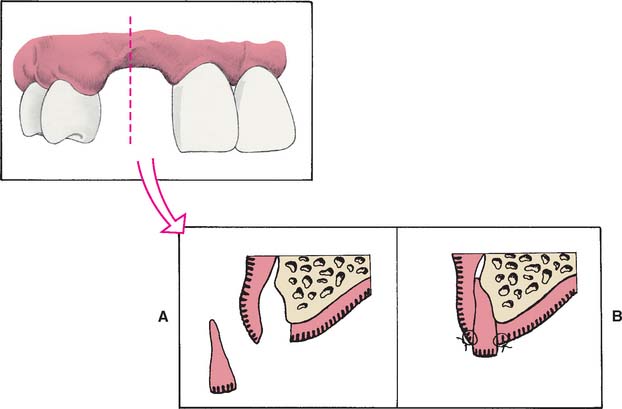
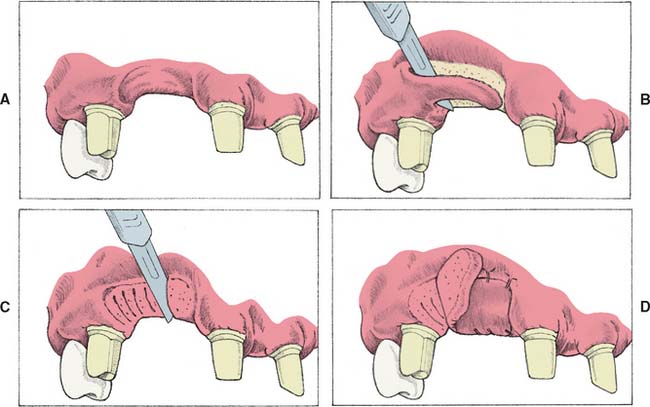
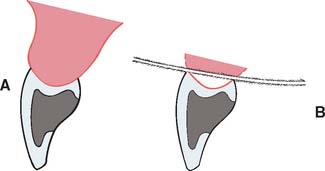
Unfortunately, few soft tissue surgical techniques can increase the height of a residual ridge with predictability. The interpositional graft2,10 is a variation of the pouch technique, in which a wedge-shaped connective tissue graft is inserted into a pouch preparation on the facial aspect of the residual ridge. The epithelial portion of the wedge may be positioned coronally to the surrounding epithelium if an increase of ridge height is desired (Fig. 20-8A and B). The onlay graft is designed to gain ridge height2,11 but also contributes to ridge width, which makes it useful for treating Class III ridge defects (Fig. 20-9). It is a thick “free gingival graft” harvested from partial- or full-thickness palatal donor sites. Because the amount of height augmentation can be only as thick as the graft, the procedure may have to be repeated several times to reestablish normal residual ridge height. Although the onlay graft has greater potential for increasing ridge height than does the interpositional graft, its survival is greatly dependent on revascularization, which requires meticulous preparation of the recipient site. Therefore, it is more technique sensitive than the interpositional graft. In fact, connective tissue grafts have been demonstrated to achieve approximately 50% more ridge volume gain 3.5 months after surgery than do free gingival grafts in single-tooth residual ridge defects.12
Gingival Architecture Preservation
Preparing the abutment teeth before the extraction is the preferred technique. An interim FDP can be fabricated indirectly, ready for immediate insertion. Because socket preservation is dependent on underlying bone contour, the extraction of the tooth to be replaced should be atraumatic and aimed at preserving the facial plate of bone. The scalloped architecture of interproximal bone forming the extraction site is essential for proper papilla form, as are facial bone levels in the prevention of alveolar collapse. If bone levels are compromised before or during extraction, the sockets can be grafted with an allograft material (hydroxyapatite, tricalcium phosphate, or freeze-dried bone).13–15
Immediately after preparation of the extraction site, a carefully shaped interim FDP is placed (Fig. 20-10A and B). The tissue side of the pontic should be an ovate form, and, according to Spear,16 it should extend approximately 2.5 mm apical to the facial free gingival margin of the extraction socket (Fig. 20-10C and D). Because the soft tissues of the socket begin to collapse immediately after the tooth extraction, the pontic causes tissue blanching as it supports the papillae and facial/palatal gingiva. The contour of the ovate tissue side of the pontic is critical and must conform to within 1 mm of the interproximal and facial bone contour to act as a template for healing. Oral hygiene in this area is difficult during the initial healing period, and so the interim restoration should be highly polished to minimize plaque retention. After approximately 1 month of healing, oral hygiene access is improved by recontouring the pontic to provide 1 to 1.5 mm of relief from the tissue. When the gingival levels are stable (approximately 6 to 12 months), the final restoration can be fabricated (Fig. 20-10E).

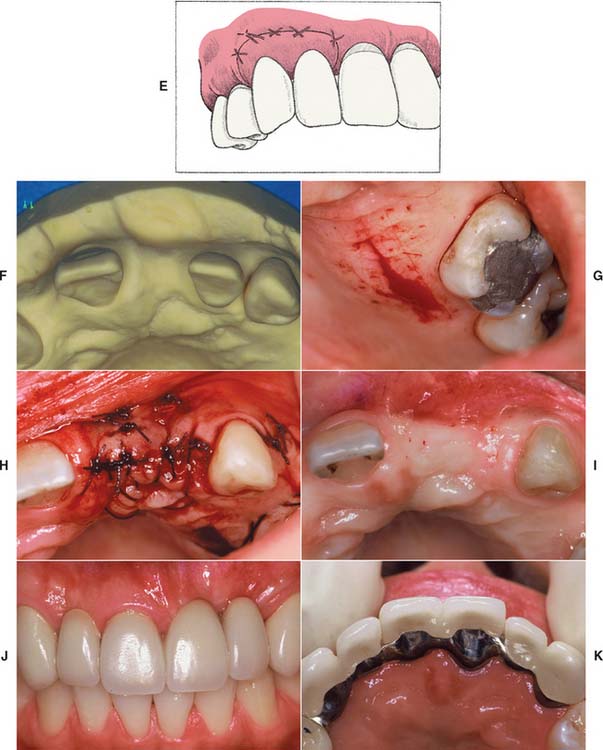
Techniques involving orthodontic extrusions have also been employed to preserve ridge form before extraction. In these proactive methods, light forces are used to extrude the teeth destined to be extracted. As the teeth are extruded, apposition of bone occurs at the root apex, thereby filling the socket with bone as the tooth is slowly extracted orthodontically. First employed to avoid ridge augmentation and gain vertical ridge height before immediate implant placement,17 the orthodontic extrusion technique has been used successfully to maintain ridge contour before treatment with conventional FDPs (Fig. 20-11). In addition to the additional time and expense of orthodontic treatment, because the teeth to be extracted must continuously be adjusted as they are extruded, previous endodontic treatment is necessary.
PONTIC CLASSIFICATION
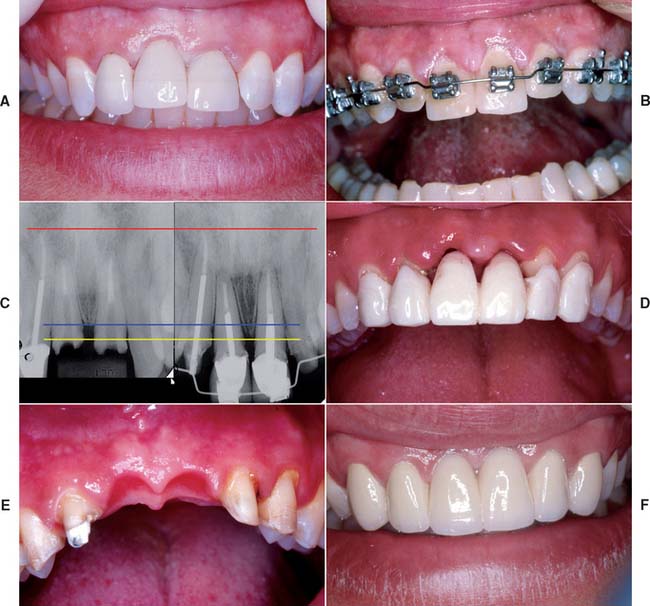
Pontic designs are classified into two general groups: those that contact the oral mucosa and those that do not (Box 20-1). There are several classifications within these groups, based on the shape of the gingival side of the pontic. Pontic selection depends primarily on esthetics and oral hygiene. In the anterior region, where esthetic appearance is a concern, the pontic should be well adapted to the tissue to make it appear as if it emerges from the gingiva. Conversely, in the posterior regions (mandibular premolar and molar areas), contours can be modified in the interest of designs that are less esthetic but amenable to oral hygiene. The advantages and disadvantages of the various pontic designs are summarized in Table 20-2.
Sanitary or Hygienic Pontic
As its name implies, the primary design feature of the sanitary pontic allows easy cleaning, because its tissue surface remains clear of the residual ridge (Fig. 20-12A). This hygienic design permits easier plaque control by allowing gauze strips and other cleaning devices to be passed under the pontic and seesawed in a shoeshine manner. Disadvantages include entrapment of food particles, which may lead to tongue habits that annoy the patient. The hygienic pontic is the least “toothlike” design and is therefore reserved for teeth seldom displayed during function (i.e., the mandibular molars).
A modified version of the sanitary pontic has been developed18 (Fig. 20-12B and C). Its gingival portion is shaped like an archway between the retainers. This geometry allows increased connector size while decreasing the stress concentrated in the pontic and connectors.19 It is also less susceptible to tissue proliferation that can occur when a pontic is too close to the residual ridge (Fig. 20-12D).
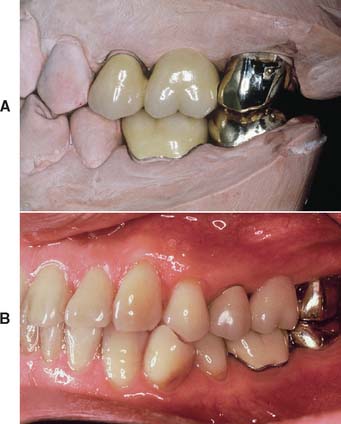
Saddle or Ridge Lap Pontic
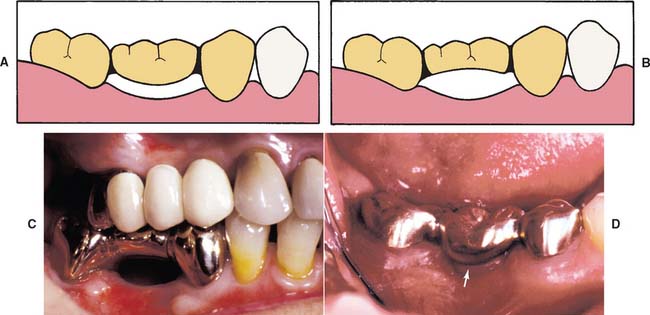
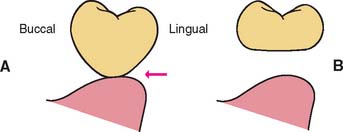
The saddle pontic has a concave fitting surface that overlaps the residual ridge buccolingually, simulating the contours and emergence profile of the missing tooth on both sides of the residual ridge. However, saddle or ridge lap designs should be avoided because the concave gingival surface of the pontic is not accessible to cleaning with dental floss, which leads to plaque accumulation (Fig. 20-13). This design deficiency has been shown to result in tissue inflammation1 (Fig. 20-14).

Modified Ridge Lap Pontic
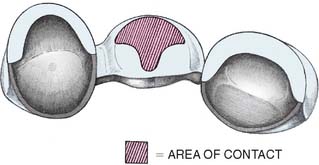
The modified ridge lap pontic combines the best features of the hygienic and saddle pontic designs, combining esthetics with easy cleaning. Figures 20-15 and 20-16 demonstrate how the modified ridge lap design overlaps the residual ridge on the facial side (to achieve the appearance of a tooth emerging from the gingiva) but remains clear of the ridge on the lingual side. To enable optimal plaque control, the gingival surface must have no depression or hollow. Rather, it should be as convex as possible from mesial to distal aspects (the greater the convexity, the easier the oral hygiene). Tissue contact should resemble a letter T (Fig. 20-17) whose vertical arm ends at the crest of the ridge. Facial ridge adaptation is essential for a natural appearance. Although this design was historically referred to as ridge-lap,20,21 the term ridge-lap is now used synonymously with the saddle design. The modified ridge lap design is the most common pontic form used in areas of the mouth that are visible during function (maxillary and mandibular anterior teeth and maxillary premolars and first molars).
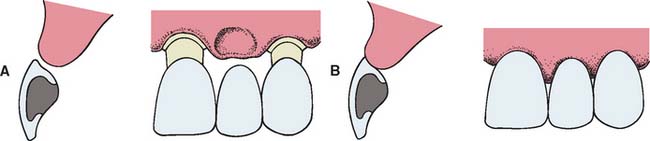
Fig. 20-15 Modified ridge lap pontic. A, Partial fixed dental prosthesis (FDP) partially seated. B, FDP seated.

Conical Pontic
Often called egg-shaped, bullet-shaped, or heart-shaped, the conical pontic (Fig. 20-18) is easy for the patient to keep clean. It should be made as convex as possible, with only one point of contact at the center of the residual ridge. This design is recommended for the replacement of mandibular posterior teeth, where esthetic appearance is a lesser concern. The facial and lingual contours are dependent on the width of the residual ridge; a knife-edged residual ridge necessitates flatter contours with a narrow tissue contact area. This type of design may be unsuitable for broad residual ridges, because the emergence profile associated with the small tissue contact point may create areas of food entrapment (Fig. 20-19). The sanitary or hygienic pontic is the design of choice in these clinical situations.
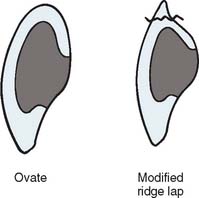
Ovate Pontic
The ovate pontic is the most esthetically appealing pontic design. Its convex tissue surface resides in a soft tissue depression or hollow in the residual ridge, which makes it appear that a tooth is literally emerging from the gingiva (Fig. 20-20). Careful treatment planning is necessary for successful results. Socket-preservation techniques should be performed at the time of extraction to create the tissue recess from which the ovate pontic form will emerge. For a preexisting residual ridge, soft tissue surgical augmentation is typically required. When an adequate volume of ridge tissue is established, a socket depression is sculpted into the ridge with surgical diamonds or electrosurgery. In either case, meticulous attention to the contour of the pontic of the interim restoration is essential when the residual ridge that will receive the definitive prosthesis is conditioned and shaped.
The ovate pontic’s advantages include its pleasing appearance and its strength. When used successfully with ridge augmentation, its emergence from the ridge appears identical to that of a natural tooth. In addition, its recessed form is not susceptible to food impaction. The broad convex geometry is stronger than that of the modified ridge lap pontic, because the unsupported, thin porcelain that often exists at the gingivofacial extent of the pontic is eliminated (Fig. 20-21). Because the tissue surface of the pontic is convex in all dimensions, it is accessible to dental floss; however, meticulous oral hygiene is necessary to prevent tissue inflammation resulting from the large area of tissue contact. Other disadvantages include the need for surgical tissue management and the associated cost. Furthermore, an additional evaluation appointment is typically necessary to achieve an esthetic result. The socket depression, with its pseudopapillae, requires the support of the interim ovate pontic and will collapse when the interim restoration is removed before an impression is made. To compensate for this three-dimensional change in the socket that occurs during the impression, it is necessary to scrape the cast in this area to ensure positive contact and support of the pseudopapillae with the definitive pontic. Because these adjustment are made somewhat arbitrarily, it may also be necessary to make revisions to the tissue surface of the pontic (reshaping or porcelain additions) at the evaluation phase.
BIOLOGIC CONSIDERATIONS
Ridge Contact
Pressure-free contact between the pontic and the underlying tissues is indicated to prevent ulceration and inflammation of the soft tissues.1,22 If any blanching of the soft tissues is observed at evaluation, the pressure area should be identified with a disclosing medium (e.g., pressure-indicating paste) and the pontic recontoured until tissue contact is entirely passive. This passive contact should occur exclusively on keratinized attached tissue. When a pontic rests on mucosa, some ulcerations may appear as a result of the normal movement of the mucosa in contact with the pontic (Fig. 20-22). Positive ridge pressure (hyperpressure) may be caused by excessive/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


