20
Plaque control and non-surgical periodontal therapy
Figure 20.1 Terms in use relating to plaque and calculus removal.

Figure 20.2 (a) Hand instruments.(b) Ultrasonic instruments.
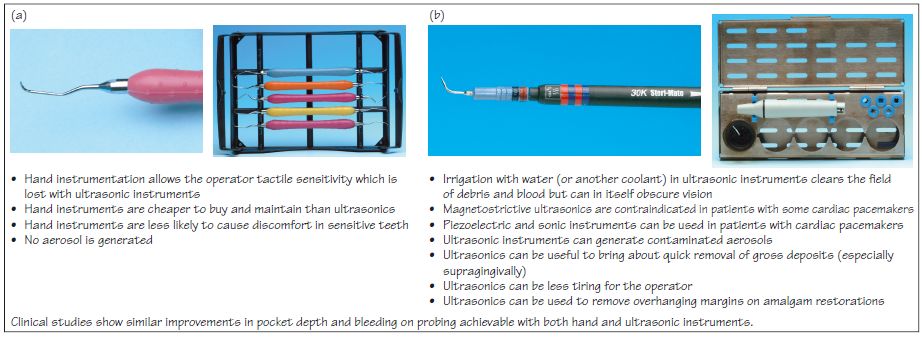
Figure 20.3 Two classic studies demonstrating the effectiveness of plaque control (Lovdal et al., 1961; Badersten et al., 1984).
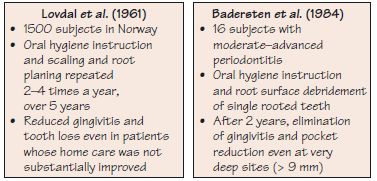
Figure 20.4 Non-surgical periodontal therapy in a 46-year-old lady with deep pockets on UR3 and UR4, which bled on probing; she experienced occlusal trauma on UR4 following extraction of UL7 and LL7. (a) UR3 probing depth (PD) of >7 mm. (b) Angular vertical infrabony defects UR3 and UR4. (c, d) Root surface debridement (RSD) of UR3 using a hoe, following ultrasonic. (e) RSD being finished on UR3 using a curette to create a clean smooth root surface; occlusal adjustment was undertaken on UR4 as part of the initial therapy. (f) PD at 2 years follow up is less than 4 mm on UR3 (shown) and UR4. (g, h) Bone level stability and corticated crest on UR3 at 2 years (g) and 5 years (h) follow up.
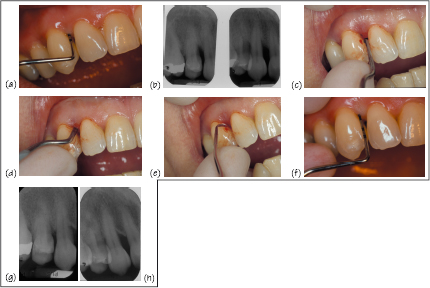
Figure 20.5 Toothbrushing advice to patient.
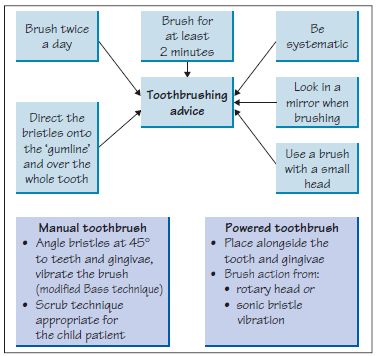
Figure 20.6 Potential use of powered toothbrushes: points to consider.
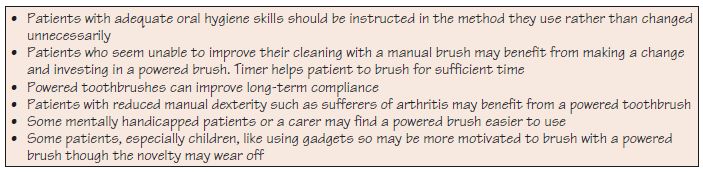
Figure 20.7 Pharmacological plaque control agents.
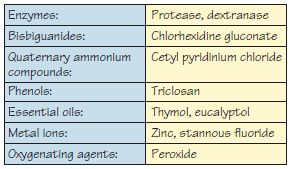
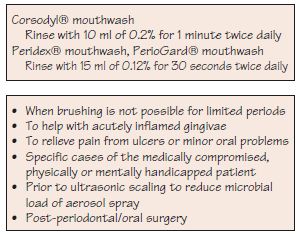
Figure 20.8 Use of chlorhexidine mouthwash.
Plaque is the primary aetiological factor in the periodontal diseases. Periodontal therapy is then directed at cleaning the root surfaces and removing plaque retention factors. Patient homecare – including toothbrushing, interdental cleaning and adjunctive pharmacological agents delivered as toothpastes and mouthwashes – is necessary after periodontal therapy to maintain the health of the periodontium. Good communication with the patient is essential to establish good hygiene practices (Chapter 21).
Non-surgical periodontal therapy
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


