Chapter 2
The Anatomy of the Root Canal System as a Challenge to Effective Disinfection
Eric Herbranson
Private practice, San Leandro, California, USA
Introduction
Nair in a 2006 review of the causes of persistent apical periodontitis in endodontically treated teeth identified six biological factors that lead to asymptomatic radiolucencies persisting after root canal treatment. These are (i) intraradicular infection persisting in the complex apical root canal system; (ii) extraradicular infection, generally in the form of apical actinomycosis; (iii) extruded root canal filling or other exogenous materials that cause a foreign body reaction; (iv) accumulation of endogenous cholesterol crystals that irritate apical tissues; (v) true cystic lesions, and (vi) scar tissue (1). He identified intraradicular infection as the main cause of unresolved apical periodontitis. The infectious agents are located in the uninstrumented recess of the internal anatomy of the root canal system and exist primarily as biofilms. The internal anatomy can be notoriously complex, especially in molars, and includes extra canals, recesses, fins, isthmuses, and accessory canals that provide space for the biofilms to reside. In addition, biofilms are difficult to eradicate. It has been reported that biofilms are a thousand times more difficult to eradicate than planktonic organisms floating in an aqueous environment (2–4). It is because of the combination of anatomical hiding places and the difficulty of destroying the biofilm that complete debridement of the canal space is probably impossible with our current treatment protocols.
The complexity of the root canal system
Root canal configuration and classification
There is great complexity and variation to the pulp space as it travels from the coronal to the apex. There are multiple canals that join and separate at unpredictable places in the tooth. All the anatomical studies from Hess forward have demonstrated this. The flatter or more ovoid the root cross-section, the greater the propensity for complexity. In the maxilla, the most variation will be found in the premolars, especially the second and the mesiobuccal (MB) root of the molars. In the mandible, anterior, premolar, and molar teeth are the ones that will show the greatest variation. The mandibular premolar is a bit of an enigma as it is usually a round root form with a single canal but it will exhibit multiple canals and great complexity on occasion. There is some ethnic variation in anatomy. For instance, blacks have the highest percentage of complex premolar, with Trope et al. (5) reporting a 32.8% incidence of two canals in the first premolar.
Weine (6) attempted to classify these into four types and later five (Figure 2.1). This was expanded by Vertucci (7) with eight different canal morphologies (Figure 2.2). These classifications were further developed by Gulabivala et al. (8, 9) to nine types, and Sert and Bayirli (10) reported an additional 14 configurations in a small subset of a Turkish population. This chasing of more and more classification points to the fundamental fact that there is great complexity in the pulp configuration in teeth. It is worth the time for a clinician to look at the Weine or Vertucci classification and then play the mental game of how one would detect, instrument, and obturate these various configurations. It will also help the clinician to appreciate the difficulty of debriding and disinfecting these shapes.
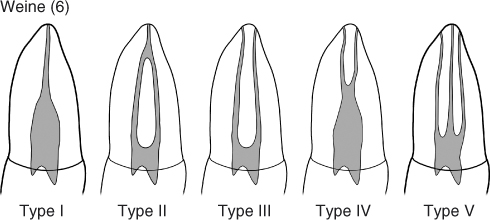
Figure 2.1 Weine’s canal classification. Originally described as four types but later expanded to five types.
(Reproduced with permission of E. Herbranson.)
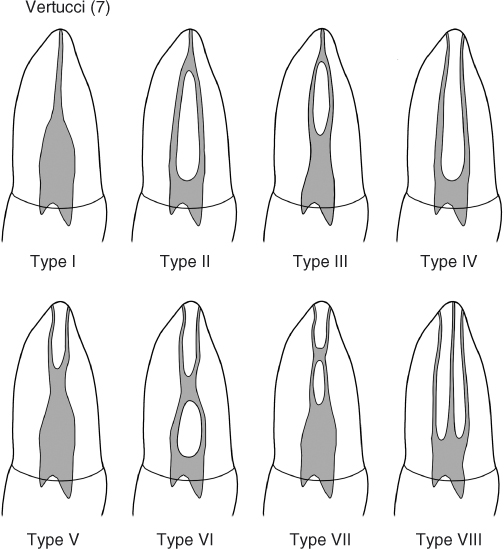
Figure 2.2 Vertucci’s canal classification.
(Reproduced with permission of E. Herbranson.)
Even with multiple angles these canal variations are difficult to detect with conventional 2D radiographs. The use of small field cone beam computed tomography (CBCT) scans are a valuable adjunct to help the clinician to detect and mentally image the canal system shape.
Root canal morphology
Pulp space shape is conceptualized by many to be a round hole. The reality is they mimic the external shape of the root. If it is round, the pulp shape will be round. If the root is ovoid, the pulp shape will be ovoid (Figure 2.3). There are a family of minor complexities in anatomy that are difficult to categorize. They include fins, niches, loops, and other oddities. They are a reflection of the unlimited variations in pulp space anatomy that exists.

Figure 2.3 A sectioned, partially developed upper first molar showing how the internal pulp space follows the external root form.
(Courtesy of Dr. David Clark.)
Accessory canals
Accessory and lateral canals extend from the pulp to the periodontium. They are found in all teeth and are formed when Hertwigs’s epithelium root sheath traps the periodontal vessels during tooth formation. Vertucci, in 1984 (7), reported their incident was 24–30% in maxillary anterior teeth, 50–60% in maxillary premolars, and 30–50% in maxillary molars with the MB root showing the highest incidence. He reported lateral canals in 18–30% of mandibular anterior teeth and almost half of lower premolars and molars. Lateral canals are found most commonly in the apical third, anywhere from 60% to 90%, with 10–16% occurring in the middle third of the root and the cervical third with a lower percentage. Complex multirooted teeth have more cervical lateral canals and may present patent accessory canals in the furcation region in 29.4% in mandibular molars, and 27.4% in maxillary molars (11).
Isthmuses and intracanal communications
Any root that has more than one canal will always present some degree of communication between those canals spaces. These features are really a variation of the complexity described by the Vertucci classification (Figure 2.4). They occur in a significant number of these types of roots with incidence as high as 71% of the maxillary first molars (12). These communications and isthmuses were respectively in 42% and 54% of the cases in the coronal third, in 59% and 79% of the cases in the middle third, and in 24% and 50% of the cases in the apical third (12). In mandibular first molars, the presence of isthmus communications averaged 54.8% on the mesial and 20.2% on the distal root (13). This anatomical communications should be taken into consideration during endodontic treatment as well as during apical surgery (14).
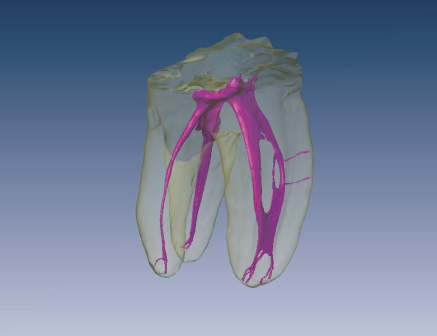
Figure 2.4 A high-resolution micro-CT scan of a three-rooted lower first molar illustrating many of the anatomical challenges facing endodontic therapy.
(Reproduced with permission of E. Herbranson.)
Figure 2.4 shows many of the complexity features discussed here illustrated in a single tooth. It has an extra root on the distolingual (DL), Vertucci type IV anatomy on the mesial root with a loop feature, later canals, and isthmus and apical deltas. All are areas for biofilm to hide in. Debridement, disinfection, and obturation of these types of spaces are difficult or impossible. This tooth could be the poster child for the anatomical challenges facing the clinician.
Apical delta
An apical delta is a pattern of small accessory canals at the apex of some teeth that looks like a river delta. The complexity and multiple portals of exit of the pulp system make these areas very hard to debride and disinfect.
C-shaped canals
C-shaped canals are an anatomic variation to keep in mind when treating maxillary and mandibular molars with adjoining or fused roots, which results in a C-shaped configuration of the canal spaces (15).
The etiology of the C-shaped canal is the fusion of the buccal aspect of the mesial and distal roots. Classification systems have been proposed by Melton et al. (16) and more recently by Fan et al. (17, 18). The anatomical variations of the C-shaped canal are numerous as the canal can vary from one distinct ribbon-shaped canal from pulp chamber to apex to three distinct separate canals with interconnections between the canals. The C-shaped canal has been reported in mandibular premolars and molars as well as in maxillary molars and its prevalence seems to be related to the ethnicity, with higher incidence of C-shaped canals in Asian populations. Zheng et al. (19) evaluated a total of 608 patients of Chinese descent with healthy, well-developed mandibular second molars and reported the presence of C-shaped canal system in 39% of the teeth.
The challenge in treating C-shaped canals lies in the thorough debridement and complete obturation because of the irregular areas of the canal house debris and necrotic tissue that is difficult to clean and fill. Mechanical instrumentation is unpredictable for disinfection, and caution should be taken when preparing the isthmus area as it is frequently very thin leading to a strip perforation. Thus, disinfection is accomplished chemically delivering and activating irrigants with ultrasonic and negative pressure irrigation with the purpose of enhancing debridement and disinfection.
The source of complexity
The anatomy complexity has its source in the development of teeth. Internal pulp anatomy is a reflection of the external anatomy of the root. This is due to the tooth formation process. Primary dentin apposition by the odontoblasts occurs at a relatively constant rate so the wall thickness of the dentin in a partially developed root will be similar around the perimeter. If the external shape is ovoid, the canal will be ovoid. If the external shape resembles a kidney bean, the internal shape will also be the same. Figure 2.3 that shows the cross-section anatomy of a partially developed upper molar illustrates this point. As the tooth reaches its full development, this kidney bean shaped root will end up with two canals with fins, inter and intracanal communications between the canals. This is shown in Figure 2.5, with the cross-sections of four MB roots of upper first molars. The three that are kidney bean shaped have two canals and isthmus anatomy. As a general rule, any tooth with a concavity in its root form has the potential for multiple canals and aberrant internal anatomy. This goes for almost all the teeth. All maxillary molars and premolars have root concavi/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


