CHAPTER 2

PORCELAIN VENEERS: YES OR NO?
MACIEJ ŻAROW

Porcelain veneers – why yes?
Are porcelain veneers a good choice? The answer is yes because they have many advantages: they are highly esthetic and look like natural teeth, and they are thin enough to let the light penetrate inside the tooth, just like alabaster or shells. In addition, preparation time is minimized, and the enamel is maintained as much as possible.
 ADVANTAGES OF VENEERS FROM A CLINICAL PERSPECTIVE
ADVANTAGES OF VENEERS FROM A CLINICAL PERSPECTIVE
 They are less invasive than prosthetic crowns1,2
They are less invasive than prosthetic crowns1,2
 There is no risk of losing pulp vitality when performing a slight preparation (enamel) (Fig 2-1)3
There is no risk of losing pulp vitality when performing a slight preparation (enamel) (Fig 2-1)3

Fig 2-1
Example of a standard preparation made under the control of a silicone index to minimize the enamel.
 Assuming that we are preparing the tooth within the enamel, the risk of hypersensitivity is minimized (Fig 2-1)4
Assuming that we are preparing the tooth within the enamel, the risk of hypersensitivity is minimized (Fig 2-1)4
 By definition, they do not interfere with periodontal tissues (juxtagingival preparation) (Fig 2-2)5
By definition, they do not interfere with periodontal tissues (juxtagingival preparation) (Fig 2-2)5

Fig 2-2a
Veneer preparation on teeth 11 and 21 with respect for the gingival margin – the juxtagingival preparation did not violate the integrity of the soft tissues.

Fig 2-2b
The preparation margin becomes visible only after inserting the first and then the second retraction cord.

Fig 2-2c
Clinical situation after veneers cementation.
 They are biocompatible and well tolerated by the gingiva, even when a minimal subgingival preparation is performed (subgingival preparation for veneers is generally not recommended. However, in some cases, it is required to cover intense discoloration or to close the black triangles in the interdental space – the veneer gently interferes with the subgingival area)5
They are biocompatible and well tolerated by the gingiva, even when a minimal subgingival preparation is performed (subgingival preparation for veneers is generally not recommended. However, in some cases, it is required to cover intense discoloration or to close the black triangles in the interdental space – the veneer gently interferes with the subgingival area)5
 They successfully improve function: symmetrical anterior guidance and lateral guidance (Fig 2-3)6
They successfully improve function: symmetrical anterior guidance and lateral guidance (Fig 2-3)6

Fig 2-3a
A 41-year-old female patient was offered four porcelain veneers in the maxillary arch, not only for esthetic reasons but also to improve anterior guidance – shown here is the clinical situation in anterior guidance before treatment.

Fig 2-3b
Four porcelain veneers were obtained.

Fig 2-3c
The patient’s smile from the semi-profile after cementation of the veneers.

Fig 2-3d
Cemented veneers from the palatal view.

Fig 2-3e
Marking the front guidance after tooth lengthening with the veneers.
 They can be redone in the future7
They can be redone in the future7
 They restore the tooth stiffness due to the physical properties of porcelain, which is important for the functional aspects of the anterior teeth8,9
They restore the tooth stiffness due to the physical properties of porcelain, which is important for the functional aspects of the anterior teeth8,9
 They can mask tooth discoloration, which is unpredictable and extremely difficult when working with composites (Fig 2-4)10–13
They can mask tooth discoloration, which is unpredictable and extremely difficult when working with composites (Fig 2-4)10–13

Fig 2-4a
Many years ago, a female patient presented to the dental office requesting to cover her teeth with veneers because multiple attempts at teeth whitening had not brought any results. The cause of the discoloration was taking tetracycline in early childhood.

Fig 2-4b
The clinical situation in the maxillary and mandibular arches.

Fig 2-4c
Ten maxillary porcelain veneers were proposed as a treatment – the photograph shows minimal veneer preparation with preservation of enamel.

Fig 2-4d
Situation after cementing porcelain veneers (feldspathic porcelain was used, now it would be possible to use “better masking” lithium disilicate porcelain).

Fig 2-4e
Patient’s smile after cementing 10 veneers in the maxilla.
 CONSIDER PLANNING PORCELAIN VENEERS WHEN:
CONSIDER PLANNING PORCELAIN VENEERS WHEN:
1. Maxillary anterior teeth have extensive, highly visible composite restorations (Fig 2-5)
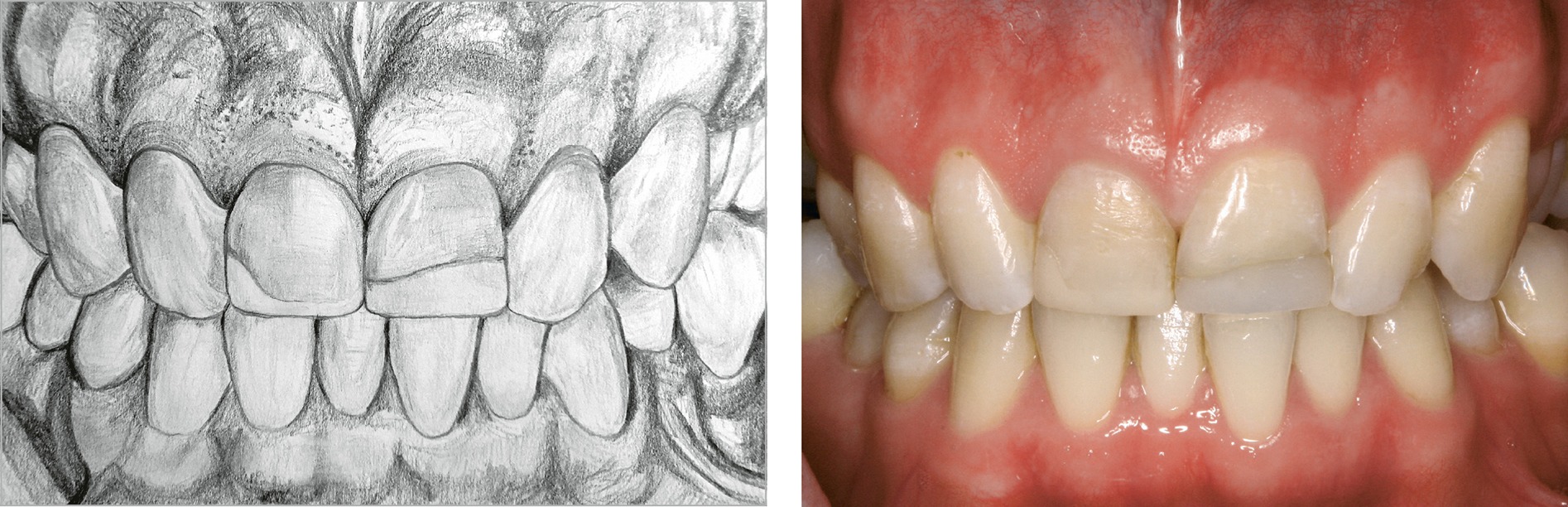
Fig 2-5
The replacement of extensive restorations can cause many difficulties, such as correct color composite matching or durability problems. In such cases, veneers can be considered.
2. Esthetic composite restorations are difficult to perform due to the need to reconstruct many teeth (Fig 2-6)
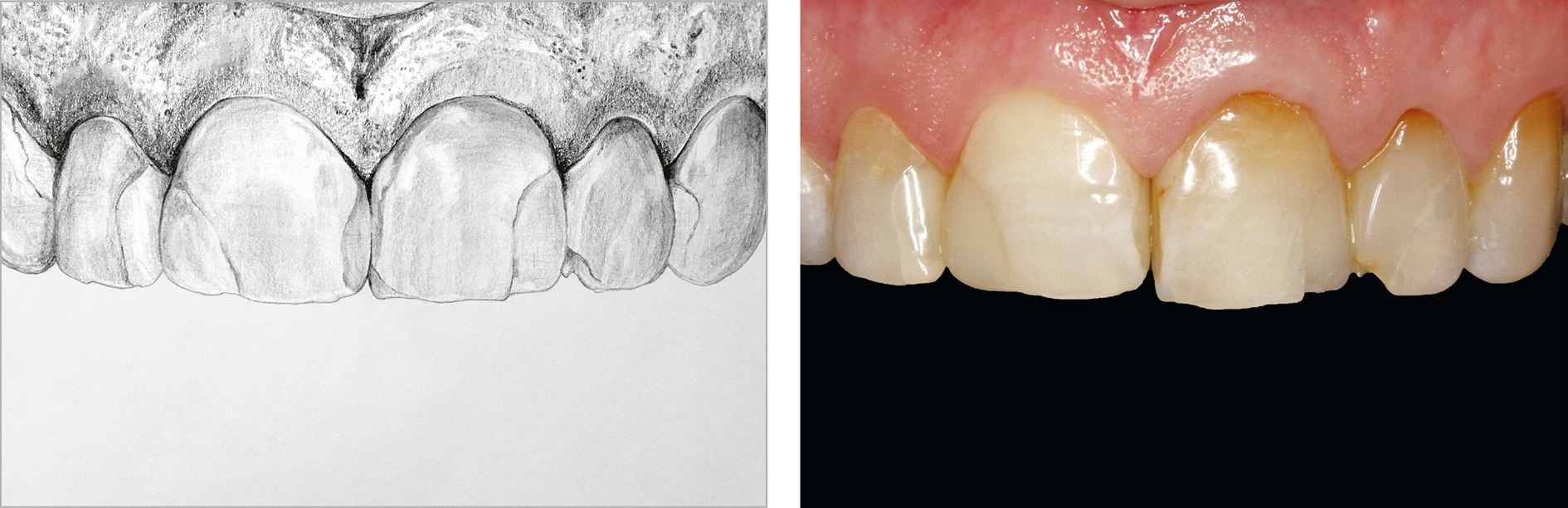
Fig 2-6
If the replacement of extensive restorations involves many teeth (for example, four or six), it is even more worth considering veneers.
Consider the advantages of porcelain veneers when you are planning esthetic treatment … but do not forget about the functional risk !
3. When a significant change of the shape or lengthening is necessary (Fig 2-7)14–16

Fig 2-7a
When maxillary central incisors are not visible in the “lips at rest” position, tooth extension should be considered for esthetic improvement. In such cases, porcelain veneers are among the treatment options.
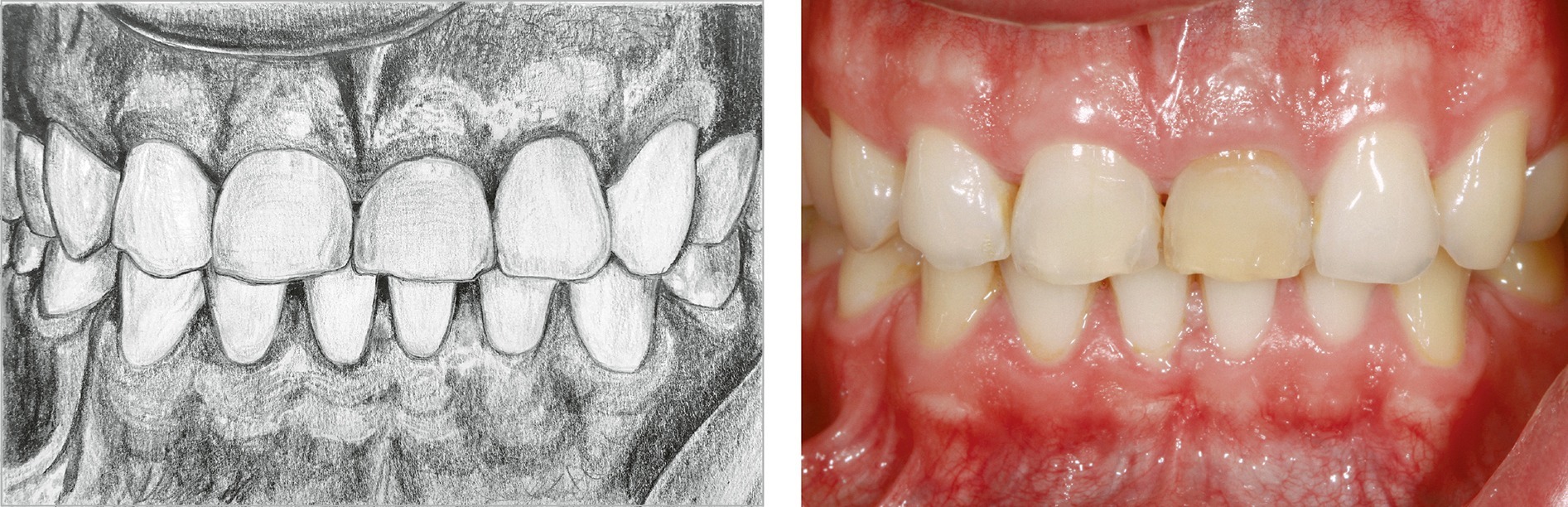
Fig 2-7b
When the maxillary central incisors have a similar length to the maxillary lateral incisors, consider changing the length or shape of the teeth to achieve dominance of the maxillary central incisors.
4. It is necessary to close the diastema (Fig 2-8)17,18

Fig 2-8
Diastema is one of the indications for porcelain veneers. However, this therapeutic option should always be analyzed individually and be visualized by mock-up before starting the treatment.
5. Reducing/closing visible black triangles (Fig 2-9)5
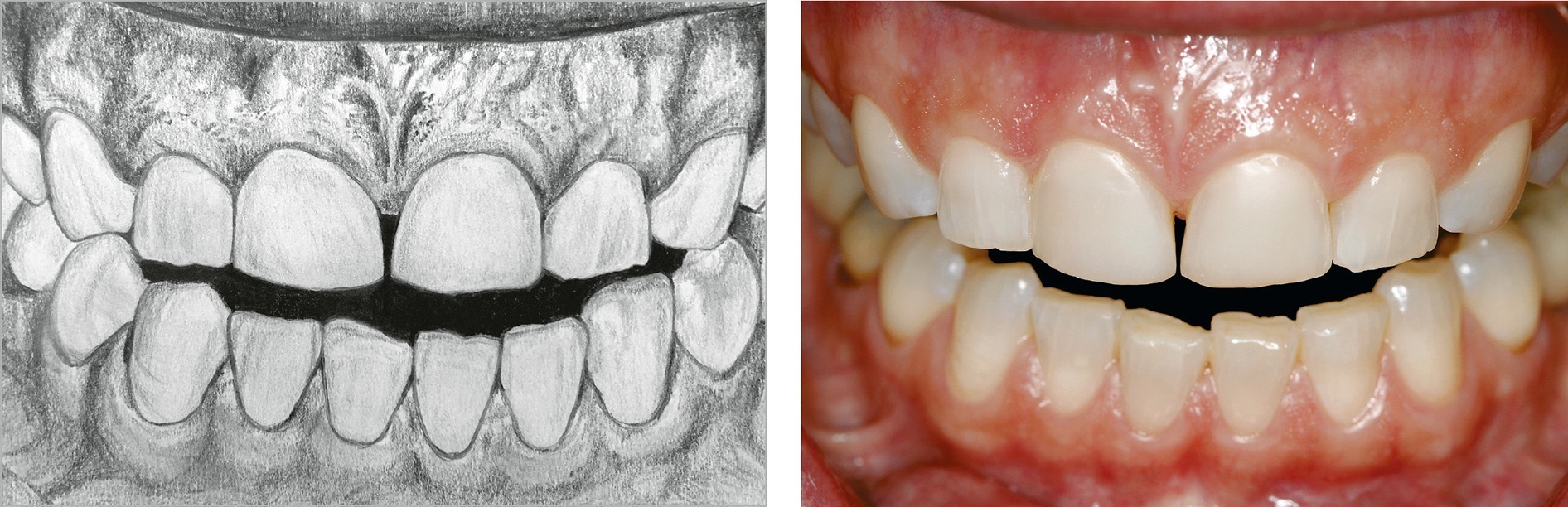
Fig 2-9
Closing black triangles is one of the indications for porcelain veneers. To achieve permanent black triangle closure, it should be done based on the knowledge of the alveolar bone position and the biological width.
6. Changing the long axis of the anterior teeth or the midline between the maxillary central incisors (Fig 2-10)5
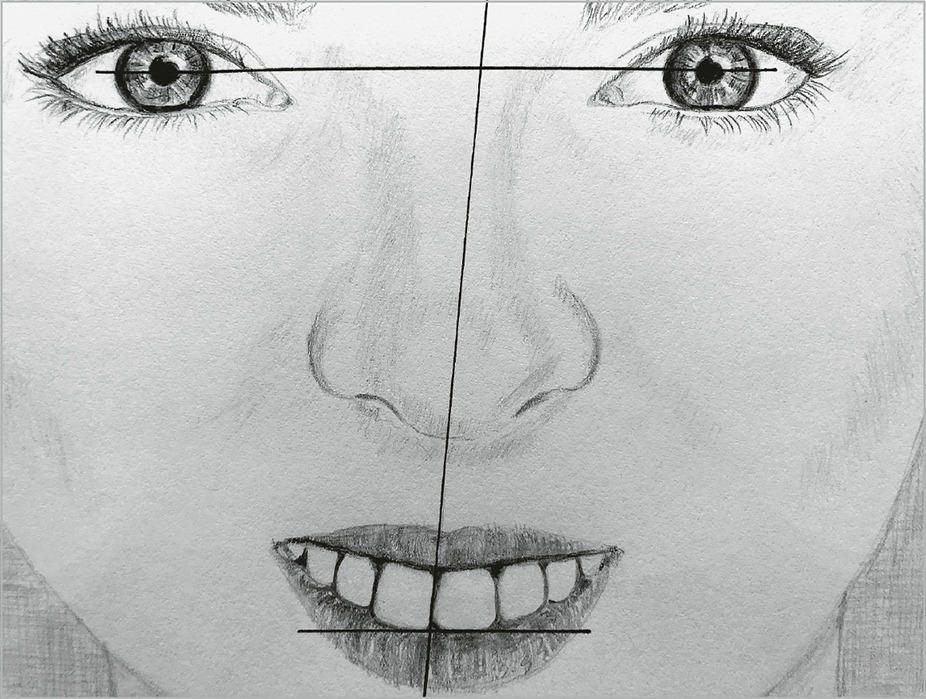
Fig 2-10
One of the indications for porcelain veneers is changing the line course between the maxillary central incisors so that it overlaps more with the facial midline and is perpendicular with the pupillary line.
 REMEMBER
REMEMBER
If you want to improve the midline course with veneers, you should plan the restoration appropriately and involve the proximal surfaces in the preparation. A photograph from the 12 o’clock position helps us understand the coincidence of a facial midline with a dental midline (see page 55, point 14).
7. Tooth is discolored and cannot be whitened or masked predictably with the composite material (Fig 2-11)19

Fig 2-11
One of the indications for making two symmetrical porcelain veneers is a discolored tooth where for some reason, internal bleaching is contraindicated, so the color cannot be masked predictably with the composite.
8. We perform a single crown and want to balance the esthetics on the other side of the dental arch (Fig 2-12)20
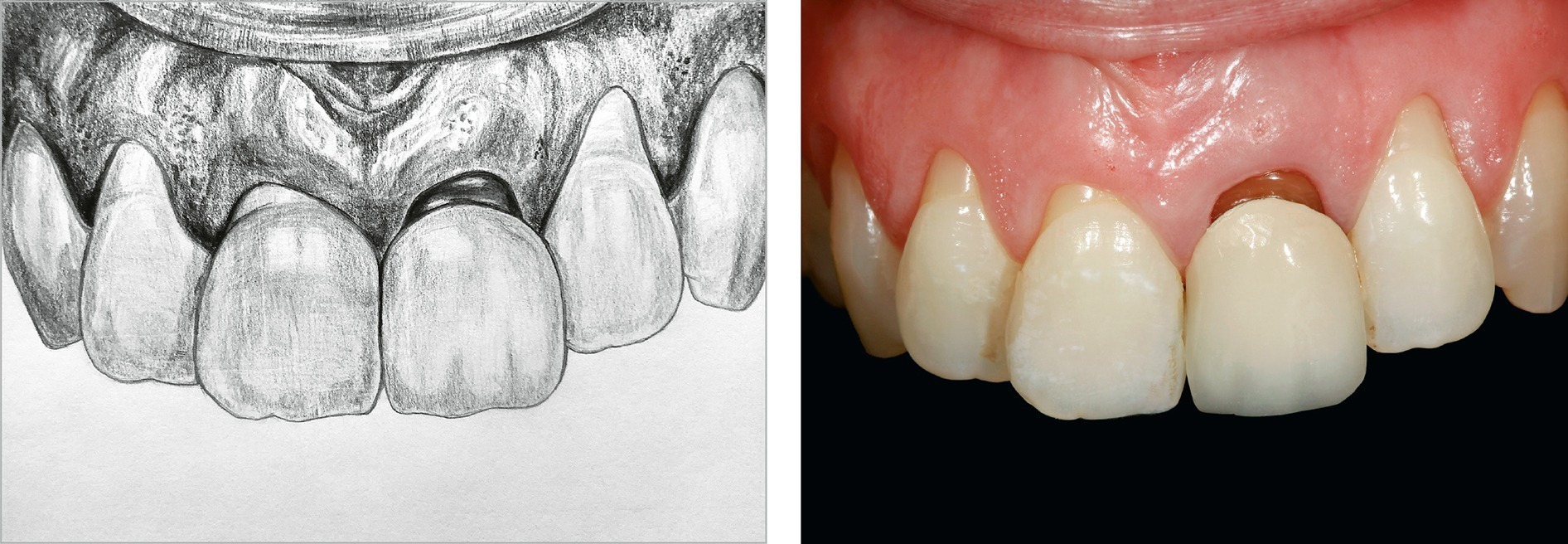
Fig 2-12
When replacing the crown on one of the maxillary central incisors, the ideal solution is to cover the symmetrically positioned incisor with a porcelain veneer made of the same porcelain as the crown.
9. When a single implant-supported crown is performed, and there is a need to balance the symmetry and to close a possible black triangle (Fig 2-13)21

Fig 2-13
When performing the maxillary central incisor implant crown, the gingival margin can change its architecture from the baseline, requiring shape change on both teeth. For this purpose, it is often necessary to carry out a veneer on the adjacent tooth.
10. When the position of the rotated tooth needs to be corrected, and orthodontic treatment is not possible for some reason (Fig 2-14)22
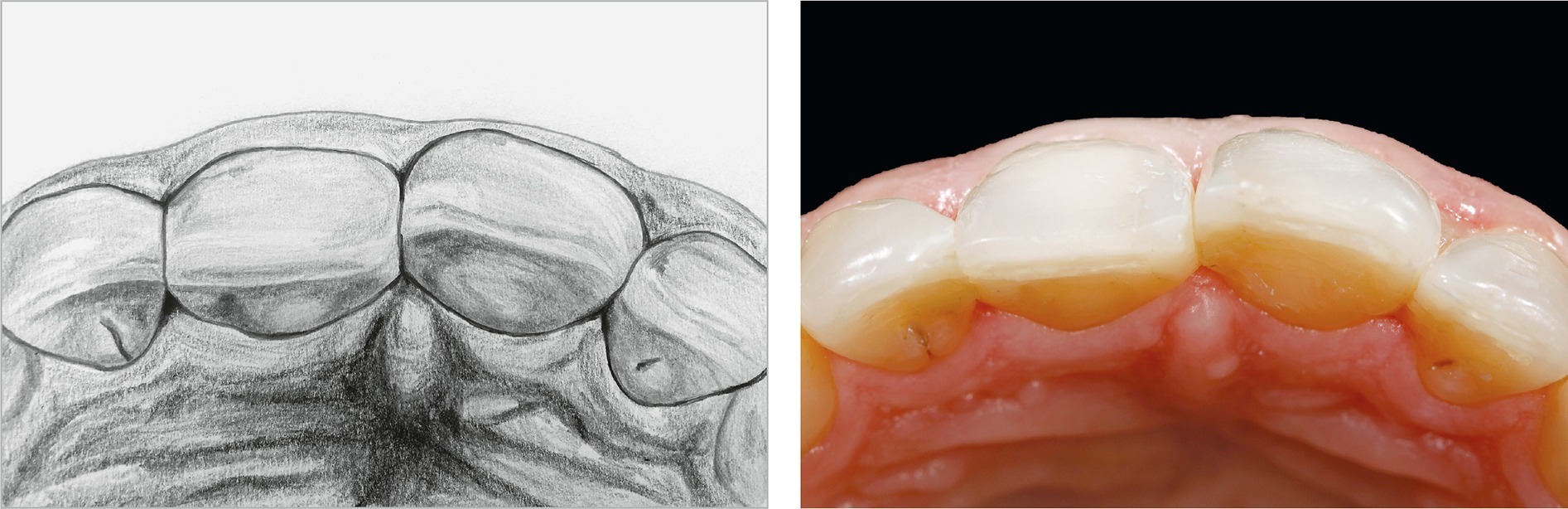
Fig 2-14
Orthodontic treatment remains the best solution for patients who require teeth aligned in the dental arch. However, it is possible to align the dental arch and improve the smile with porcelain veneers in some cases, especially when the teeth position enables us to minimize tooth preparation.
11. When complex occlusal rehabilitation is planned – as the last step of restoring the function and esthetics in the anterior segment (Fig 2-15)23

Fig 2-15
In cases like this, porcelain veneers are indicated but usually only after reconstruction of the occlusion by creating appropriate space for restorative material in the anterior teeth.
Porcelain veneers – why no?
You cannot agree to even very convincing suggestions from patients who are absolutely sure that porcelain veneers are the only possible treatment. The clinical situation and indications should be realistically assessed. Sometimes, even the greatest efforts can lead to months of disputes and resentments.
 DO NOT PLAN PORCELAIN VENEERS WHEN:
DO NOT PLAN PORCELAIN VENEERS WHEN:
1. There is a small amount of tooth structure, and less than 50% of the tooth structure would adhere to the veneer after preparation (Fig 2-16)13

Fig 2-16
Two different clinical situations. (a) There is enough tooth structure in teeth 11 and 21. (b) After veneer preparation in tooth 11, less than 50% of the hard tissues will be left, and in tooth 21, the quantity of hard tissues will be around 50%. Therefore, the replacement of fillings or ceramic crowns should be considered. It is possible to make porcelain veneers in this case, but the risk of failure in the future (for example, cracks) increases significantly when the veneer has a composite build-up on most of its preparation surface.
If more than 50% of the hard tissues remain after veneer preparation, we can expect proper adhesion and durability for such reconstruction. The more enamel, especially on the margins of the preparation, the better chance for a long-lasting marginal seal. The same is true for the ratio of tooth structure to composite surface within the preparation. Although similar to tooth tissues (especially to dentin), composite behaves slightly differently over the years. It shows a tendency to water sorption and volume change, which means that the veneer may “work” differently when it is bonded to the hard tissue surface and the composite surface.
This will not matter for small composite restorations,13 but it is difficult to predict how the veneer will behave when the base surface is a large Class 4 restoration.
Suppose we add a lack of stable occlusion and bilateral support on the lateral teeth or constricted chewing pattern. In that case, the total of the unfavorable factors becomes even greater.
2. There are subgingival cavities or Class 5 restorations reaching the cementum (Fig 2-17)24
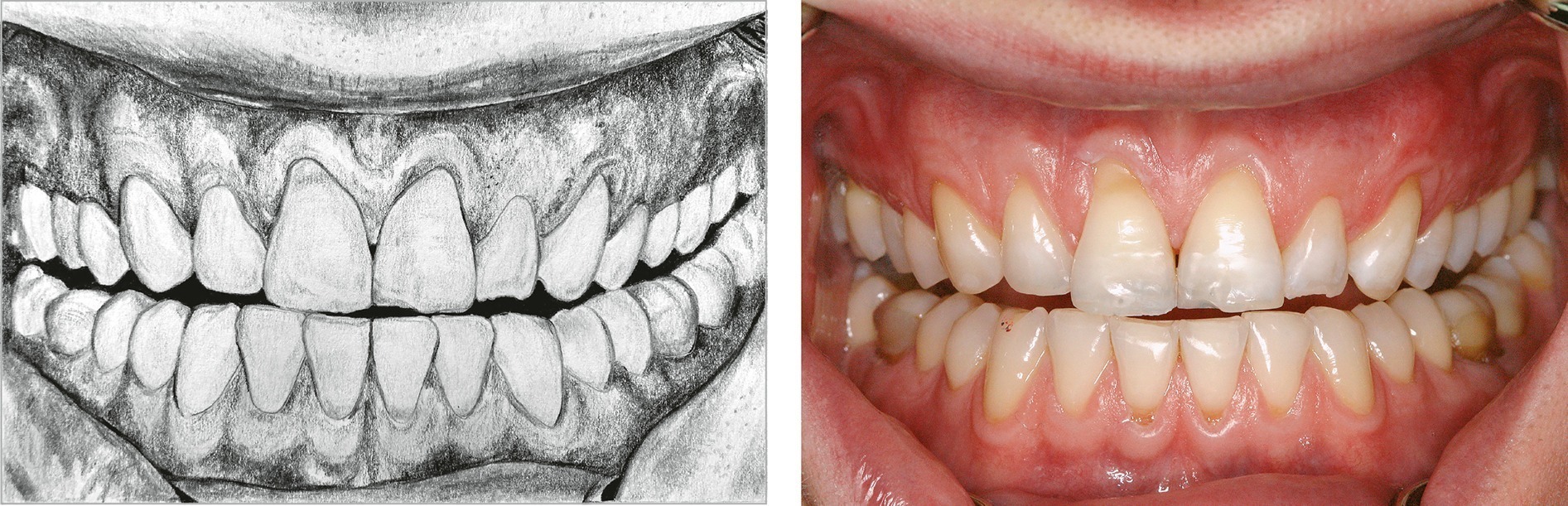
Fig 2-17
When cavities reach the cementoenamel junction and interfere in the cementum zone, the risk of the veneer entering the cementum should be taken into account (faster aging of the adhesion and risk of stress accumulation).
When Class 5 composite restorations are placed subgingivally deep enough that placing a rubber dam to control the moisture and removing excess material during cementation is not possible, veneers are contraindicated. In addition, the cervical part of the veneer is a critical zone in terms of stress distribution. The cervical area of the tooth accumulates much stress: this is where the enamel reaches the cementum (cementoenamel junction, CEJ), and main types of non-carious cervical lesions are formed, ie, abfractions (due to occlusal overload).
If the margin of the preparation can be located in the enamel in this critical gingival zone, the durability of the veneer will increase. If a significant part of the preparation is located subgingivally in the cementum, the veneer’s adhesion to the tooth will decrease critically. In addition, it will not be possible to control moisture during cementation or to remove excess material.
For these reasons, the marginal seal of the veneer and periodontal health will be unpredictable. The location of the veneer margin on the composite in the gingival zone is contraindicated in the case of an existing Class 5 restoration. The veneer may cover the entire filling, but the gingival margin should not finish on the restoration but on the tooth structure.
 REMEMBER
REMEMBER
If the gingival margin of the veneer preparation is located deep subgingivally, the long-term marginal seal of the veneer and periodontal health will not be predictable. In such a clinical situation, think about alternative solutions such as direct or indirect composite restorations. In the event of chipping or other problems, they can be repaired!
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


