2
Patient Selection for Implant Therapy: Oral Systemic Health, Medical History, and Risk Assessment
The terms oral health and general health should not be interpreted as separate entities. Oral health is integral to general health; this report provides important reminders that oral health means more than healthy teeth and that you cannot be healthy without oral health.
—Surgeon General Report, 2001
Over the past 30 years, implantology and periodontal medicine have changed the way we think about dentistry. Dental professionals have moved away from the examination for decayed or broken teeth to a comprehensive examination of the entire mouth and overall health of the patient. The traditional dentistry resolution for missing teeth was to do nothing, bridge, or partial or full removable denture. After 15 years of wearing a denture, patients can suffer from gastrointestinal disorders from reduced ability to chew their food and this may lead to a shorter life expectancy (1). Partial denture wearers often experience the “domino” effect, losing the teeth that support the partial at a rate of 44% within 10 years (2). There are even romantic consequences for edentulous patients, as they can be reluctant to start new relationships, and some edentulous patients are categorized as oral invalids unable to wear their dentures without pain (3). Today, the optimal restorative options for replacing missing teeth are implants.
It is an exciting time to be in dentistry, with the increasing use of regeneration/implant therapy, and hygienists play an important role. Hygienists are recommending, assessing, maintaining, and monitoring implants. Implants rank second only to bleaching procedures as the most asked about treatment in dentistry. As hygienists we hold the key to many of the relationships of our patients to the practice. Often, we are asked, “What should I do to replace this tooth? What are my options?” We must be aware of what to look for in a potential implant patient and what makes a patient contraindicated for implant dentistry. Keep in mind that many implant candidates are dental failures, periodontal disease patients, or patients with poor oral health habits.
The best candidates for implants are your existing patients of record. You have patients with missing teeth, partials, dentures, and bridges that are failing. You already have a relationship and trust with these patients. Another key source of implant candidates is referrals from your existing satisfied implant patients. Don’t be afraid to ask for referrals from your satisfied patients to encourage more patients that are of “like mind” to come to your office.
Patient selection for implants is based on a number of factors including oral systemic health, medical history, risk assessment, and hygiene status. Patients who are immunosuppressed or taking anticoagulants, steroids, or IV bisphosphonates can be contraindicated for implant therapy. Heavy smokers, poorly controlled diabetics, patients with previous poor bone-healing history, and patients with multiple systemic health problems should be evaluated carefully. Any diseases that can directly affect the ability of osteoblasts to lay bone or interfere with wound healing of bony tissue are contraindicated for placement of implants.
Uncontrolled diabetics and heavy smokers are at the top the list of contraindicated patients due to the poor vascularization of the gingival tissues as well as higher risk for infection and slower healing time. However, a controlled diabetic is an ideal implant patient due to the added benefit of implant dentistry that the implants do not decay.
A smoker can also be a good candidate for implant therapy if he or she first attends a smoking cessation program and agrees to the risks associated with possible loss of the implant. Immunosuppressed patients, such as HIV-positive patients, who want to improve digestion can be considered for implants, but would need to be controlled and monitored.
Age, osteoporosis, and periodontal bone loss may also be an obstacle that can be hurdled. Periodontal maintenance patients who are compliant with home care can be excellent candidates but should be placed on 3-month recall for implant maintenance. The same bacteria that caused the periodontal disease will still be present in their oral cavity.
If the patient’s medical history indicates that he or she has any of these potential contraindications, the dental hygienist should always check with the dentist prior to recommending implants to these patients to determine whether or not the patient would be a good implant candidate on a case-by-case basis. If a patient asks, review all the options and let the patient know that the doctor will determine if he or she is a candidate for implant therapy.
An edentulous patient at any age can benefit from implant dentistry; there is no cut-off age. As a general rule, it is recommended that growth has been completed prior to implant placement for children younger than 16 years of age, but children can be considered for implants on an individual basis.
The hygienist is ideal to assist the dentist in the selection process to determine the patient’s motivation, dexterity for home care necessary for the selected treatment, and expectations of therapy outcome, as well as to identify patients with risk factors, habits, and conditions that place patients at a higher risk for implant failure.
The patient’s aesthetic and functional expectations have a direct correlation to the number of implants necessary, type of restoration to be used, time to heal, and how much the final cost of treatment will be. All of these factor into patient selection and need to be discussed with the patient prior to treatment.
A complex or larger treatment case may require a separate treatment conference to be scheduled with the doctor and/or implant coordinator to walk the patient through the treatment options, time involved, and fees associated with the case. The doctor may also need to collaborate with the patient’s physician prior to proceeding with implant therapy due to a systemic health factor.
The selection process for implant therapy is interdisciplinary and the hygienist needs to have an understanding of oral systemic health, medical history, and risk factors to help identify potential implant candidates.
Oral systemic health link to overall health
It is now widely accepted and research confirmed there is an oral systemic connection: a link established between bacterial infections, oral bacterial biofilm, and cytokine release in periodontal tissues. The link between oral infection and certain systemic diseases has taken center stage, and inflammation is the key!
Who better to identify inflammation than hygienists who evaluate for potential periodontal disease on a daily basis? Periodontal disease is one of the major inflammatory diseases in the body. Dental professionals, therefore, hold a key role not only in the treatment of periodontal disease and peri-implant disease, but in comprehensive disease management.
Periodontal medicine is now the coined term that looks at the risk for certain systemic diseases that is increased by an oral infection (e.g., periodontal and peri-implant disease) from patients’ inflammatory response to infection.
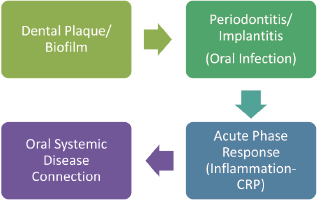
To fully understand the severity of the problem, a basic knowledge of how bacteria from the periodontal or peri-implant sulcus gains access to the systemic circulation (i.e., blood stream) is important. The bacterial biofilm comes in contact with ulcerated epithelium, which creates a pathway directly to the systemic circulation. Gram-negative bacteria, which are always present in the oral cavity, have access to the blood vessels, which allows the infection to reach other tissues and organs throughout the body. Periodontal and/or peri-implant disease act as a reservoir of pro-inflammatory mediators or modules that enhance the inflammatory response. They enter the systemic circulation and can induce and/or perpetuate systemic effects that can ultimately affect the overall health of the patient (see Figure 2.1).
Figure 2.1 Inflammation process.
There are four major diseases with proven links to periodontal disease: cardiovascular/cerebrovascular disease, preterm birth/low birth weight, diabetes, and respiratory disease; see Box 2.1.
Cardiovascular/Cerebrovascular (CV/CV) disease: The link between periodontal disease and cardiovascular disease/stroke results from the changes caused by infection and/or inflammation responses that affect the build up of plaque on the inner lining of the blood vessels supplying the heart (coronary arteries) or brain (carotid arteries) that occur in atherosclerosis (4, 5). According to the Academy of Periodontology Mouth Body Connection, “Researchers have found that people, especially diabetics with periodontal disease are almost twice as likely to suffer from coronary artery disease.”
Preterm birth/low birth weight: Studies have proven a link between periodontal disease/infection and the risk of adverse pregnancy outcomes, including preterm birth and low-weight babies (48–50). This is caused by the action of blood-borne oral bacteria or an increase in the blood levels on the inflammatory mediators that cause early delivery.
Diabetes: Periodontitis is a proven complication and all patients with diabetes should be evaluated for periodontal disease and monitored for signs of infections in the periodontium of implants. Diabetics have a decreased ability to fight off bacterial infections. The bacteria invades the gingiva, which can lead to infections and bone loss (51). Diabetes mellitus also affects the severity and rate of progression of periodontitis, and might increase the risk of poor metabolic control (52, 53).
Respiratory disease has been linked to periodontal disease and inflammation and is particularly prevalent in patients in nursing homes and institutionalized individuals, those who need assistance to maintain good oral hygiene. Periodontal infection and respiratory pathogens in plaque have been linked to an increased risk for aspiration pneumonia and some studies suggest chronic obstructive pulmonary disease (COPD) (54).
Cardiovascular/cerebrovascular (CV/CV) disease
There is a documented association between periodontal disease/infection and the risk for CV/CV disease. The national survey of health conditions of the United States population collected between 1988 and 1994 (NHANES III database) “states the relationship between periodontal attachment loss and the risk of myocardial infarction was demonstrated.” These data suggest a real and important influence of periodontitis on the risk of CV/CV disease.
As dental professionals we can provide treatment for periodontitis/implantitis that may help prevent the onset of and delay of the progression of CV/CV disease. Oral bacteria and plaque can affect the heart by attaching to fatty plaques in the arteries and form clots. These clots can cause obstructions that can lead to a heart attack. Infection and/or inflammation responses can also affect the build up of plaque on the inner lining of the blood vessels supplying the heart (coronary arteries) or brain (carotid arteries) that occur in atherosclerosis (4, 5).
Growing numbers of research studies also support the contribution of periodontal infection to the inflammatory burden theorized to be through both a direct action on blood vessel walls, and by indirectly inducing the liver to produce cardiac reactive proteins (CRP) through an acute-phase response (6). It is produced by the liver in response to infection and inflammation, and is a specific systemic marker of vascular inflammation that appears to have a strong association with adverse vascular events; see Figure 2.1 (7).
Cardiac reactive proteins are also referred to as hepatic plasma proteins or C-reactive proteins. They are found in trace amounts in even healthy people, however, if elevated levels of these proteins are found it can signify serious inflammation in the body. CRP levels can go as high as 400–500 mg/L in seriously ill patients (see Table 2.1). Many different diseases and conditions can elevate CRP levels; such as periodontal disease, cardiovascular disease, trauma, surgery, burns, advanced malignancy, Alzheimer’s disease, blood sugar disorders, smoking, and obesity.
Table 2.1 Levels of cardiac reactive protein (CRP).
| Normal CRP | <1.0 mg/L |
| Intermediate CRP | 1.0–2.9 mg/L |
| High CRP | >3.0 mg/L |
Alzheimer’s disease is being viewed as an inflammatory brain disorder due to studies that have shown that patients with high levels of CRP were three times more likely to develop Alzheimer’s disease. Tobacco also raises CRP levels and has a residual affect that remains in the body for years. Smoking causes oxidants to form and might accelerate the oxidation of LDL’s constituents, which causes arterial inflammation even in healthy individuals with normal LDL levels.
To identify and monitor inflammation, the CRP simple blood test is becoming a leading marker for systemic inflammation in the body. Intermediate to high levels of CRP found in this specific blood test indicate an increase in inflammation somewhere in the body and are cause for concern.
CRP testing has the potential to become a significant tool for identification of patients at risk for CVD and prevention of CVD (8). Dental professionals are currently using high-sensitivity C-reactive protein (hsCRP) testing in dental practices chair-side or requesting the test from the patient’s physician to identify patients at risk for acute coronary syndromes and to monitor periodontal disease.
Severe periodontal disease patients have more harmful bacteria in their blood streams than patients with moderate or no disease (Figure 2.1). The inflammatory process of periodontal disease increases CRP levels and when periodontal disease or peri-implant disease are treated, the CRP levels decrease and the haemoglobin A1c (HbA1c) levels improve (9, 10). HbA1c level is also an important marker in monitoring diabetes. Both CRP and LDL cholesterol level tests are minimally correlated, but CRP has been found in some studies to be a stronger predictor of future cardiovascular events than LDL cholesterol (7).
For this reason, Healthy Heart Dentistry, a blood testing company for dental offices in the United States, has a combination test for CRP and HbA1c levels. The QuikRead® CRP (Orion Diagnostica) is a simple test for quantitative determination of CRP and is also available from Mirage Medex in the United Kingdom; see the Appendix for testing company information.
The bottom line is that CRP are going to be an important link for dentistry. Inflammation is turning out to be the missing link for diagnosing and treating many systemic diseases. The key for dentistry is that periodontal disease and now peri-implant disease is one of the most prominent inflammatory diseases in the bod/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


