Medical history, examination, investigations and risk assessment
Key Points
• Crucial history-taking includes (A–E):
1. allergies
4. drug history
5. endocrine disease (e.g. diabetes)
• Patients may be unclear about, or unaware of or not disclose their medical history or drug history
Protecting Patients
Health care aims to improve the health of patients but can itself carry risks. The first principle should be to do no harm (primum non nocere). Nevertheless, a UK report estimated that up to 18% of the population believe that they have suffered from a ‘medical error’, 10% of hospital admissions may result in something going wrong and 5% have had adverse effects from medical care. In a survey of Dutch oral surgeons who had had, on average, 21 years of work experience, 40% of respondents confirmed that they had experienced the death of a patient after oral surgery. Most of these patients had died after a dental extraction, the most important causes of death being postoperative spread of an infection, failure to survive cancer treatment, or heart and/or lung failure.
Operations are now associated with far less morbidity and mortality than formerly but there remains room for improvement. Morbidity and mortality in the dental surgery providing local anaesthesia (LA) and conscious sedation (CS) are rare but greater in patients with medical and/or dental problems; for example, extractions attributed to dental infections were significant predictors for risk factors for myocardial infarction compared with tooth extraction for trauma and other reasons in an Oslo study. Deaths as a result of the use of general anaesthesia (GA) in the dental surgery in the past were few but nevertheless provoked widespread public concern, and it is no longer permissible for a dentist in the UK to act as anaesthetist (this had been the case for some time in some other countries). GA must only be given in a hospital with critical care facilities – because of the need to have resuscitation equipment available – and must be carried out by a qualified anaesthetist.
If working in hospital, however, dentists may be required to assess patients for GA and to ensure that essential prerequisites are met before GA, and may need to manage GA patients postoperatively. They must therefore have an understanding of risk assessment and perioperative care.
Risk Assessment
At the start of a patient’s visit, it is essential to:
2. assess the patient’s needs and agree them with the patient
3. obtain the patient’s valid consent to any investigations required
4. obtain the patient’s consent to an agreed treatment plan.
Adequate risk assessment is essential and endeavours to anticipate and prevent trouble. The criteria of ‘fitness’ for a procedure are not absolute but depend on a number of factors, as shown in Box 2.1. Dentistry should be very safe, especially if the procedure is not dramatically invasive and the patient is healthy.
Surgical procedures are generally the most hazardous. The World Health Organization (WHO) recognizes this and grades risks on the basis of severity of the procedure (Table 2.1). WHO also identifies three phases of an operation at each of which, for patient safety, a checklist coordinator must confirm that the surgery team has completed the listed tasks before it proceeds:
■ Before anaesthesia induction (‘sign in’)
■ Before skin incision (‘time out’)
■ Before the patient leaves the operating room (‘sign out’).
Table 2.1
| Grade | Termed | Includes |
| 1 | Minor | Excision of skin lesion; drainage of breast abscessa |
| 2 | Intermediate | Primary repair of inguinal hernia; excision of varicose vein(s) of leg; tonsillectomy/adenotonsillectomy; knee arthroscopy |
| 3 | Major | Total abdominal hysterectomy; endoscopic resection of prostate; lumbar discectomy; thyroidectomy |
| 4 | Major+ | Total joint replacement; lung operations; colonic resection; radical neck dissection; neurosurgery; cardiac surgery |
Drug use is also potentially dangerous; all agents should be carefully administered, particularly those acting on the neurological system and affecting consciousness and cardiac or respiratory functioning (e.g. sedatives and anaesthetic agents). Most oral care is given under LA and then morbidity is minimal. CS is not as safe as LA, though considerably safer than GA. Even so, CS must be carried out in appropriate facilities, by adequately trained personnel and with due consideration of the possible risks. By contrast, GA with intravenous or inhalational agents is only occasionally required for dental treatment and then only in a hospital setting; control of vital functions is impaired or lost to the anaesthetist. As stated above, GA is only permitted in a hospital with appropriate resuscitation facilities.
A patient attending for dental treatment who is apparently ‘fit’ may actually have serious systemic disease(s) and be taking drugs (including recreational drugs), either or both of which might influence the health care required. Many patients with life-threatening diseases now survive as a result of advances in surgical and medical care, and either or both can significantly affect the dental management or even the fate of the patient. Though this is most likely when treating hospital patients and other risk groups such as older people, one study showed that 30% of dental patients have a relevant medical condition. The risk is greatest when surgery is needed, and when GA or CS are given – and these problems may be compounded if close medical support is lacking.
Although every care must be taken to identify the medically compromised patient, it must be appreciated that the means to do so in conventional dental settings are limited and by no means always successful. It is impossible to legislate for all possibilities and there have been many cases where apparently fit people have died suddenly within a short time of being declared healthy on medical examination.
The main aims are to ensure that procedures are carried out:
However, although risks arise mainly when the procedure is invasive (tissues are disrupted) and/or the patient is not healthy, they may also be a factor if health-care professionals (HCPs) are overambitious in terms of their skill or knowledge. Clinicians should work only within their field of competence. No interventional procedure is entirely free from risk but care can be improved by making an adequate assessment based on history, clinical signs and, where appropriate, investigations, and by minimizing trauma and stress to the patient (Table 2.2).
Table 2.2
Risk assessment and management
| Risks increased by | Risks reduced by |
| Increasing age | Planned treatment |
| Medical treatments | Non-invasive procedures |
| Surgical treatments | Monitoring |
| Lengthy dental procedures | Reassurance |
| Drug use – medication or recreational | Competent operator |
Assessment of the risks involved must include the health of the patient, which may be evaluated using a risk-stratification scoring system such as the Physical Status Classification of the American Society of Anesthesiologists (ASA) (Table 2.3). ASA I and II patients can generally be treated in general dental practice or community services. ASA III patients are often best treated in a hospital-based clinic where expert medical support is available. ASA IV and V patients are usually hospitalized or bedridden, and generally are only seeking emergency dental treatment.
Table 2.3
American Society of Anesthesiologists (ASA) classification
| ASA class | Definition |
| I | Normal, healthy patient |
| II | A patient with mild systemic disease (e.g. well-controlled diabetes, asthma, hypertension or epilepsy), pregnancy, anxiety |
| III | A patient with severe systemic disease limiting activity but not incapacitating (e.g. epilepsy with frequent seizures, uncontrolled hypertension, recent myocardial infarct, uncontrolled diabetes, severe asthma, stroke) |
| IV | A patient with incapacitating disease that is a constant threat to life (e.g. cancer, unstable angina or recent myocardial infarct, arrhythmia or recent cerebrovascular accident) |
| V | Moribund patient not expected to live more than 24 h with or without treatment |
Dental treatment must be significantly modified if the patient has an ASA score of III or IV, which is true of a relatively high percentage of patients aged 65–74 years (23.9%) and 75 years or over (34.9%). Controversies can arise in relation to the management of patients with ASA scores of II and III. Table 2.4 summarizes these scores for some of the more common disorders.
Table 2.4
American Society of Anesthesiologists (ASA) grades II and III
| ASA II | ASA III | |
| Chronic obstructive pulmonary disease (COPD) | Cough or wheeze; well controlled | Breathless on minimal exertion |
| Angina | Occasional use of glyceryl trinitrate (GTN) | Regular use of GTN or unstable angina |
| Hypertension | Well controlled on single agent | Poorly controlled; multiple drugs |
| Asthma | Well controlled with inhalers | Poorly controlled; limiting lifestyle |
| Diabetes | Well controlled; no complications | Poorly controlled or complications |
The Prognosis and Assessment of Risk Scale (PARS) is another assessment tool, which is virtually identical to the ASA scale but can be modified by factors such as those shown in Table 2.5; it categorizes patients into groups I–V. Other factors considered in PARS are shown in Table 2.6. The Karnofsky scale, which has been adapted for use in many areas including hospices, cancer clinics and so on, is a quick and easy way to indicate how a patient is feeling on a given day, without going through several multiple choice questions or symptom surveys (Table 2.7). The Medical Complexity classification is another available tool (Table 2.8).
Table 2.5
< ?comst?>
| ASA | Definition | PARS | Dental care modifications |
| I | Normal, healthy patient | I | None |
| II | A patient with mild systemic disease (e.g. well-controlled diabetes, asthma, hypertension or epilepsy), pregnancy, anxiety | II | Dental care should focus on elimination of acute infection before medical/surgical procedure (e.g. prosthetic cardiac valve) |
| III | A patient with severe systemic disease limiting activity but not incapacitating (e.g. epilepsy with frequent seizures, uncontrolled hypertension, recent myocardial infarct, uncontrolled diabetes, severe asthma, stroke) | III | Dental care should focus on elimination of acute infection and chronic disease before medical/surgical procedure (e.g. organ transplant patients) |
| IV | A patient with incapacitating disease that is a constant threat to life (e.g. cancer, unstable angina or recent myocardial infarct, arrhythmia or recent cerebrovascular accident) | IV | All potential dental problems should be corrected before medical/surgical procedure (e.g. prior to radiotherapy to head and neck) |
| V | Moribund patient not expected to live more than 24 h with or without treatment | V | Control of acute dental pain and infection only |
< ?comen?>< ?comst1?>

< ?comst1?>
< ?comen1?>
Table 2.6
Prognosis and Assessment Risk Scale
| Factor | Comment |
| Medical status | Any complicating medical factors |
| Physical status | |
| Oral hygiene | |
| Psychological needs | |
| Functional ability | |
| Mental status | Level of understanding |
| Social environment | Support or significant events planned shortly after treatment |
| Family environment | |
| Access issues | Access to dental building, etc. |
| Financial issues | |
| Communication needs | Is an interpreter required? |
| Behaviour | Is behaviour management needed? |
| Consent | Is patient competent to give consent? |
Table 2.7
| Score | Definition |
| 100 | Able to work. Normal, no complaints, no evidence of disease |
| 90 | Able to work. Able to carry out normal activity, minor symptoms |
| 80 | Able to work. Normal activity with effort, some symptoms |
| 70 | Independent, not able to work. Cares for self, unable to carry out normal activity |
| 60 | Disabled, dependent. Requires occasional assistance, cares for most needs |
| 50 | Moderately disabled, dependent. Requires considerable assistance and frequent care |
| 40 | Severely disabled, dependent. Requires special care and assistance |
| 30 | Severely disabled. Hospitalized, death not imminent |
| 20 | Very sick. Active supportive treatment needed |
| 10 | Moribund. Fatal processes are rapidly progressing |
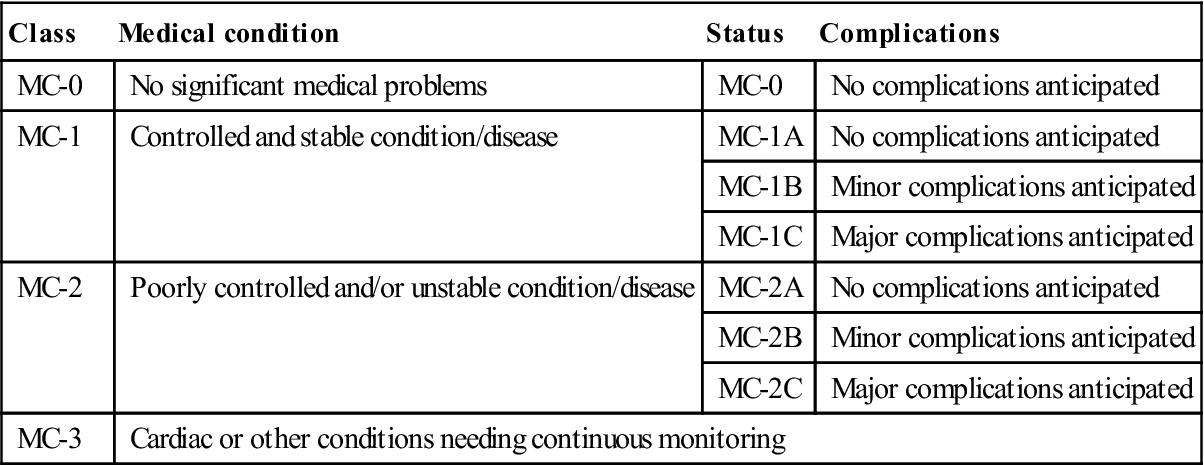
Table 2.8
Medical Complexity classification
< ?comst?>
| Class | Medical condition | Status | Complications |
| MC-0 | No significant medical problems | MC-0 | No complications anticipated |
| MC-1 | Controlled and stable condition/disease | MC-1A | No complications anticipated |
| MC-1B | Minor complications anticipated | ||
| MC-1C | Major complications anticipated | ||
| MC-2 | Poorly controlled and/or unstable condition/disease | MC-2A | No complications anticipated |
| MC-2B | Minor complications anticipated | ||
| MC-2C | Major complications anticipated | ||
| MC-3 | Cardiac or other conditions needing continuous monitoring | ||
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
Good communication is essential with both patient and other health professionals. Often, dental treatment in medically compromised patients may have to be delayed until expert advice has been sought and this is always the case for patients undergoing procedures under GA, who must be pre-assessed by the anaesthetist.
Informed Consent (otherwise known as valid consent)
The patient’s autonomy must be respected at all times. Patients can determine what investigations and treatment they are or are not willing to receive. Before they are asked to make a decision, they must be given sufficient information about their condition, suggested treatment(s) (including alternative management if available), any associated risks involved in the proposed treatment, and possible outcomes if nothing is done. They have the right to refuse treatment, even if this could adversely affect the outcome or result in their death. Depending on the situation, time should be allowed for the patient to think about and discuss the proposed treatment with people close to them. Consent is the expressed or implied agreement of the patient to undergo an examination, investigation or treatment. Consent is not an isolated event, but involves a continuing dialogue between clinician and patient (and occasionally their relatives or partner). In order to give informed (valid) consent, the individual concerned must have adequate reasoning faculties and be in possession of all relevant facts at the time consent is given. Patients who undergo procedures performed without their valid consent may be entitled to claim damages in the civil courts by making a claim of negligence. The clinician is also vulnerable in the criminal courts to a charge of assault and battery following a complaint to the police by the person who received the treatment.
Information about what the proposed investigations or treatment will involve, the benefits and risks (including adverse effects and complications), and the alternatives available is crucial for patients when they are making up their minds. The courts have stated that patients should be told about ‘significant risks which would affect the judgment of a reasonable patient’.
‘Significant’ has not been legally defined but the General Medical Council (GMC) requires doctors to tell patients about ‘serious or frequently occurring’ risks. In addition, if patients make it clear that they have particular concerns about certain kinds of risk, the clinician must ensure that they are informed about these risks, even if they are very small or rare. Sometimes, patients may make it clear that they do not want any information about the options, but want the health professional to decide on their behalf. In such circumstances, ensure that the patient receives at least some very basic information about what is proposed. Where information is refused, this should be documented in the patient’s notes and/or on a consent form. The important thing is for the clinician to record sufficient details of the consent process in order to be able to reconstruct the discussions and the thinking that led to a particular course of treatment in the event of a challenge at a later stage – possibly years later.
The patient’s open agreement to proceed with the investigation or treatment proposed after full discussion and the patient’s receipt of sufficient information is sometimes called ‘informed consent’.
When obtaining consent, patients should be informed of:
■ details of the diagnosis and prognosis with and without treatment
■ uncertainties about the diagnosis
■ options available for treatment
■ the purpose of all aspects of a proposed investigation or treatment
■ the likely benefits and probability of success
■ any possible adverse effects and the risks of the procedure proposed
■ the likelihood of one or more of the risks coming to pass
■ likely outcomes if a procedure is not carried out
■ the need for drains, catheters, tracheostomy, etc.
Other issues that should be discussed at this stage include:
■ time of appointment or admission
■ eating/starving instructions
■ management of usual daily medications
■ specific preoperative preparation that may be required
■ transport to where the procedure will be performed
‘Informed’ consent means that the patient must be fully aware of the procedure, its intended benefits and its possible risks, and the level of these benefits and risks. In particular, patients must be warned about:
All questions should be answered honestly. Information should not be withheld that might influence the decision-making process. Patients should never be coerced. Finally, for consent to be valid, the person who obtains it must have sufficient knowledge of the proposed treatment and its risks, and should be the person who is undertaking the procedure.
At any time, the information on the form can be augmented by an additional record made in the patient’s notes covering conversations, discussions or warnings.
Although rarely a legal requirement (but frequently a contractual obligation), it is good practice to seek written consent on most occasions and this is essential where the treatment is complex or involves significant risks or adverse effects. Written consent must always be obtained from all patients having an operation. The possible benefits of the treatment must be weighed against the risks and always discussed by the person carrying out the procedure; if, for some reason, this is not possible, it must be done by a delegated person with the appropriate expertise to do so (i.e. a person who is competent to carry out the proposed surgery themselves as an independent practitioner in their own right). Written consent is also essential when provision of clinical care is not the primary purpose, the treatment is part of a project or research, or there are significant consequences for personal or social life. Your organization may have a policy setting out when you need to obtain written consent. A signature on a consent form does not itself prove the consent is valid; the point of the form is to record the patient’s decision and also, increasingly, the content of the discussions that have taken place. A signed consent form is not a legal waiver; if, for example, patients do not receive enough information on which to base their decision, then the consent may not be valid, even though the form has been signed. A signed consent form will not protect the clinician if there is doubt as to whether consent was actually ‘informed’. Ideally, the form should be designed to serve as an aide-mémoire to health professionals and patients, by providing a checklist of the kind of information patients should be offered, and by enabling the patient to have a written record of the main points discussed. However, the written information provided for the patient in no way should be regarded as a substitute for face-to-face discussions with the individual. Patients are also entitled to change their mind after signing the consent form, if they retain capacity to do so.
Although the law in relation to consent continues to evolve (as does most legislation) and there are significant variations between countries, the principles are as follows:
■ Before examining, treating or caring for competent adults, consent must be obtained.
■ Adults are assumed to be competent unless demonstrated otherwise.
For consent to be valid, patients must receive sufficient information about their condition and proposed treatment. It is the HCP’s responsibility to explain all the relevant facts to the patient and to ascertain that they are understood. If there are doubts about their competence, the question to ask is: ‘Can this patient understand, retain and then weigh up the information needed to make this decision?’ If patients are not offered as much information as they reasonably need to make their decision, and in a form they can understand, their consent may not be valid. For example, information for those with visual impairment should be provided in the form of audio tapes, Braille or large print.
Patients whose first language is not English may need the help of an interpreter. Most organizations have access to experienced interpreters. It is preferable to rely on a neutral interpreter (i.e. not a family member) when examining and seeking consent from a patient for surgery or treatment.
Ensure the patient, staff and, where appropriate and in accordance with the patient’s wishes, the patient’s relatives and/or partner are kept fully informed. Maintain good, clear, contemporaneous records of the nature of all discussions that take place, including the names of those involved. Good communication and documentation can prevent future dispute and litigation. If there is any reason to believe that consent may be disputed later, or if there are concerns about an individual’s attitude or behaviour, meticulous documentation in the case notes is essential. The UK Department of Health’s Reference guide to consent for examination or treatment (available at www.gov.uk/government/publications; accessed 30 September 2013) offers a comprehensive summary of the law on consent.
Specific Consent Issues
■ No one else can make a decision on behalf of a competent adult.
■ In an emergency, a life-saving procedure can be performed without consent.
■ All actions must, however, be justifiable to one’s peers.
■ No one can give or withhold consent on behalf of a mentally incapacitated patient; decisions lie primarily with the clinicians, who should act in the patient’s best interest. Where there is doubt, ultimately a court will decide on the best course of action, having taken expert advice. The Mental Capacity Act 2005 provides guidance for HCPs in England and Wales (see also The Adults with Incapacity (Scotland) Act 2000) who treat this group of patients. Guidance has been published by the UK Department of Health (Mental Capacity Act 2005 Code of Practice) and is available at http://www.dca.gov.uk/legal-policy/mental-capacity/mca-cp.pdf (accessed 30 September 2013).
Essentially, everyone aged 16 or more is presumed to be competent to give consent for themselves, unless the opposite is demonstrated.
Competent adults – namely, persons aged 16 and over who have the capacity to make their own decisions about treatment – can consent to dental treatment and they are also entitled to refuse treatment, even where it would clearly benefit their health. If a patient is mentally competent to give consent but is physically unable to sign a form, you should complete this form as usual and ask an independent witness to confirm that the patient has given consent orally or non-verbally.
If the patient is 18 or over and is not legally competent to give consent, you should use a form for adults who are unable to consent to investigation or treatment. Patients will not be legally competent to give consent if:
■ they are unable to comprehend and retain information material to the decision; and/or
■ they are unable to weigh and use this information in coming to a decision.
You should always take all reasonable steps (e.g. involving more specialist colleagues) to support patients in making their own decision before concluding that they are unable to do so.
Relatives cannot be asked to sign this form on behalf of an adult who is not legally competent to consent for him or herself, unless the patient has appointed a friend or relative to act for them, creating a lasting power of attorney (LPA). This LPA must have been created when the patient was competent and the LPA must be lodged with the Court of Protection. An LPA may allow the relative or friend to take decisions about the health of the patient, should the patient be found to be lacking capacity.
Children under the age of 16 years may also have capacity to consent if they have the ability to understand the nature, purpose and possible consequences of the proposed investigation or treatment, as well as the consequences of non-treatment. Children below 16 who have Gillick competence (i.e. they understand fully what is involved in the proposed procedure) may therefore consent to treatment without their parents’ authority or knowledge, although their parents will ideally be involved. ‘Gillick competence’ is a term used in medical law to decide whether a child (16 years or younger) is able to consent to medical treatment, without the need for parental permission or knowledge:
As a matter of Law the parental right to determine whether or not their minor child below the age of sixteen will have medical treatment terminates if and when the child achieves sufficient understanding and intelligence to understand fully what is proposed.
The standard is based on a House of Lords’ decision in the case Gillick v West Norfolk and Wisbech Area Health Authority [1985] 3 All ER 402 (HL). The case is binding in England, and has been approved in Australia, Canada and New Zealand. Similar provision is made in Scotland by the Age of Legal Capacity (Scotland) Act 1991. In Northern Ireland, although separate legislation applies, the then Department of Health and Social Services Northern Ireland stated that there was no reason to suppose that the House of Lords’ decision would not be followed by the Northern Ireland Courts.
Where a child under 16 years old is not deemed competent to consent, a person with parental responsibility (e.g. their legal parent or guardian, or a person appointed by the courts) has authority to consent for investigations or treatment that are in the child’s best interests.
There are several legal tests that have been described in relation to consent. The Bolam test states that a doctor who:
acted in accordance with a practice accepted as proper by a responsible body of medical men skilled in that particular art is not negligent if he is acting in accordance with such a practice, merely because there is a body of opinion which takes a contrary view.
However, a judge may, on certain rare occasions, choose between two bodies of expert medical opinion, if one is to be regarded as ‘logically indefensible’ (Bolitho principle). The main alternative to the Bolam test is the ‘prudent-patient test’ widely used in North America. According to this test, doctors should provide the amount of information that a ‘prudent patient’ would want.
Obtaining consent from adult patients without capacity
The more elective the procedure, the more care should be taken in ensuring that the patient, parent, guardian or carer has been consulted. In true emergency situations, a dentist may rely on the best-intent principle in relation to the overall well-being of the patient, although, where there is any doubt, advice should be taken. Involve the patient as far as possible; some incapacitated patients may be quite capable of giving partial consent. Decide who else should be involved in any decision to proceed with the patient’s treatment. The current position (in the UK) is that no adult can consent to the treatment of another adult (with the exception of cases that fall under the Mental Capacity Act 2005). Before anyone can give valid consent to treatment, she or he must possess the requisite capacity. The law presumes that, in the absence of evidence to the contrary, patients over the age of 16 years are capable of giving (or withholding) consent to treatment. The broad test of capacity is that the person concerned should be able to understand the nature and purpose of the treatment and must be able to weigh the risks and benefits. They should be able to retain and weigh this information, as well as communicate their decision.
Where there is doubt, a decision has to be made as to the capacity of the patient. This presents a problem for dentists providing care for patients with learning impairment. Where the patient lacks the capa-city to consent, then the dentist would normally act in the patient’s best interests and treatment should not be withheld simply because consent has not been obtained, or a charge of failure in duty of care could be made. If a person is incapable of giving or refusing consent, and has not validly refused such care in advance, treatment may still be given lawfully if it is deemed to be in the patient’s best interests. However, this should happen only after full consideration of its potential benefits and unwanted effects, and in consultation with the carer(s), relatives and other people close to the patient. Where treatment involves taking irreversible decisions or carrying greater risks, then the agreement of another dentist or doctor is appropriate. For those with learning difficulties, it is important to have a discussion with the parent, carer or, in their absence, two professionals who should sign their approval in the best interests of the patient. The discussions and agreement should be documented in the patient’s record and, whilst this does not constitute consent, it represents good practice.
The Mental Health Act 1983 is primarily concerned with the care and treatment of people who are diagnosed as having a mental health problem which requires that they be detained or treated in the interests of their own health and safety or with a view to protecting other people.
The Mental Capacity Act 2005 applies to everyone involved in the care, treatment or support of people aged 16 years and over in England and Wales who lack capacity to make all or some decisions for themselves. This Act also applies to situations where a person may lack capacity to make a decision at a particular time due to illness, drugs or alcohol. Assessments of capacity should be time- and decision-specific. The Act clarifies the terms ‘mental capacity’ and ‘lack of mental capacity’, and says that a person is unable to make a particular decision if they cannot do one or more of the following:
■ Understand information given to them
■ Retain that information long enough to be able to make the decision
A new criminal offence of ill-treatment or wilful neglect of people who lack capacity also came into force in 2007. Within the law, ‘helping with personal hygiene’ (that would include tooth-brushing) attracts protection from liability, as long as the individual has complied with the Act by assessing a person’s capacity and acting in their best interests. ‘Best-interest’ decisions made on behalf of people who lack capacity should be the least restrictive of their basic rights and freedoms.
Further changes within the Act include the introduction of LPAs that extend to health and welfare decisions. When a health professional has a significant concern relating to decisions taken under the authority of an LPA that relate to serious medical treatment, the case can be referred for adjudication to the Court of Protection, which is ultimately responsible for the proper functioning of the legislation. The Act also created a new Public Guardian with responsibility for the registration and supervision of both LPAs and court-appointed deputies. Furthermore, Independent Mental Capacity Advocates (IMCAs) have been introduced to support particularly vulnerable incapacitated adults – most often those who lack any other forms of external support – in making certain decisions.
In Scotland, the position is complicated by the fact that the dentist has to comply with the Adults with Incapacity Act 2000. This requires the patient’s doctor to issue a certificate before treatment. The document is procedure-specific and a new one is required for each treatment plan or in the event of a change to the plan. Episodes requiring GA or sedation not included in the original treatment plan will need further certification. The interesting nuance is that the dentist can assess capacity but it is the doctor who has to assess incapacity. This has created significant practical difficulties for many health-care providers.
Obtaining consent for child patients
Changing social patterns have meant that the position relating to who is able to consent to treatment for a child is no longer the same. Parental responsibility lies with the natural mother, natural father (if married to the mother at birth), adoptive parents or those who have temporary residence orders (where the child lives with them). The local authority may acquire responsibility. The natural father not married to the natural mother does not have parental responsibility. Parental responsibility can be granted by court order, by agreement with the mother or on her death, if stated in her will. Step-parents can be granted parental responsibility by court order.
It is important to remember that the legal situation with regard to consent varies around the world and is subject to continued debate and development.
The Use of Restraint
Occasionally, patients may need some assistance in order to be able to undergo or cooperate with investigations or treatment. The dividing line between assistance and trespass to the person can be fine. Three forms of trespass to the person exist:
■ Assault – the fear or threat of impending harm
■ Battery – the unlawful application of force or unwanted touching
These issues must be considered carefully when the patient lacks the necessary capacity to understand the procedure being carried out. Any physical intervention is subject to the rule of ‘reasonableness’. Sometimes it is necessary to control movements during operative procedures or to support an arm, for example, for the injection of intravenous drugs in order to prevent patients injuring themselves. It is wise to seek the assistance of a carer or relative at such times and to ensure that this is documented. Learning disabilities teams may be able to assist and are likely to have developed protocols and procedures to deal with such problems.
Medical History
The history (or anamnesis) is the information gained by an HCP with the aim of formulating a diagnosis, providing medical care and identifying medical problems relevant to health care. The history is obtained from either the patient or people who know the patient and can provide the necessary information. History-taking also allows the HCP to develop rapport with the patient, place the diagnosis in the context of the patient’s life, identify relevant physical signs, and assess mental state and attitude towards health care. Age and cultural factors may also be important (Appendices 2.1 and 2.2). Due cognisance must be taken of a person’s “protected characteristics”, of which there are nine (Table 2.9).
Table 2.9
| Age | Where this is referred to, it refers to a person belonging to a particular age (e.g. 32 year olds) or range of ages (e.g. 18–30 year olds). |
| Disability | A person has a disability if s/he has a physical or mental impairment which has a substantial and long-term adverse effect on that person’s ability to carry out normal day-to-day activities. |
| Gender reassignment | The process of transitioning from one gender to another. |
| Marriage and civil partnership | Marriage is defined as a ‘union between a man and a woman’. Same-sex couples can have their relationships legally recognised as ‘civil partnerships’. Civil partners must be treated the same as married couples on a wide range of legal matters. |
| Pregnancy and maternity | Pregnancy is the condition of being pregnant or expecting a baby. Maternity refers to the period after the birth, and is linked to maternity leave in the employment context. In the non-work context, protection against maternity discrimination is for 26 weeks after giving birth, and this includes treating a woman unfavourably because she is breastfeeding. |
| Race | Refers to the protected characteristic of Race. It refers to a group of people defined by their race, colour, and nationality (including citizenship), ethnic or national origins. |
| Religion and belief | Religion has the meaning usually given to it but belief includes religious and philosophical beliefs including lack of belief (e.g. Atheism). Generally, a belief should affect your life choices or the way you live for it to be included in the definition. |
| Sex | A man or a woman. |
| Sexual orientation | Whether a person’s sexual attraction is towards their own sex, the opposite sex or to both sexes. http://www.equalityhumanrights.com/advice-and-guidance/new-equality-act-guidance/protected-characteristics-definitions/ |
It may occasionally be helpful to carry out a formal assessment of the patient’s feelings about health care, and tools such as the Corah anxiety scale are available for this (Box 2.2; Ch. 10).
When taking a history, a structured guide such as that shown in Box 2.3 should be followed. Patients should also be given a form on which to supply all the information they can about their health and any medication they are receiving. Medical and drug history should be regularly updated at subsequent dental visits. Remember that all such information is confidential.
Personal Details
The patient’s personal details include age, sex, educational status, religion or faith, occupation, relationship status, address and contact details. This information is necessary for administrative purposes and, since the questions are largely non-threatening, this stage provides a gentle introduction into the meeting of patient and clinician, in a format that can be individualized to suit a particular culture.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


