2
Medical Emergencies
In the past, oral health-care practitioners might have expected to encounter one life-threatening situation among their patients during years of practice. With advances in medicine, and the prevalence of dental disease in a geriatric patient population, the clinician may now be called on more often to provide dental care to medically and/or pharmacologically compromised patients. Being ill-prepared for such eventualities is inexcusable. Being the subject of public censure or accused of negligence in the office is an agony best prevented. Assessment of the patient and recognition of actual or potential problems are imperative in initiating proper treatment and/or summoning proper help. A system of patient classification adopted by the American Society of Anesthesiologists (Table 2-1), with the primary purpose of quickly and easily placing each patient in an appropriate risk category, can provide guidelines for the course of patient management. This classification must be made during the physical evaluation of the patient before any dental treatment is initiated.
Consequently, oral health-care providers must be able to recognize high-risk patients and initiate immediate correction of life-threatening problems. Although there are a number of techniques available for maintaining life in emergency situations, many require sophisticated devices and valuable time that the patient simply may not have. Oral health-care providers must know how to sustain life with no more than their hands, their breath, a few basic supplies and therapeutic agents, and a great deal of common sense.
Table 2-1 Risk Status Classification for Dental Patients
| Risk Status | Definition | Approach |
|---|---|---|
| I | No overt systemic condition(s) | Routine office care |
| May require sedation | ||
| II | Moderate systemic condition(s) | Routine office care |
| Medically stable | Appropriate minor modifications | |
| III | Severe systemic condition(s) | Emergency care |
| Medically fragile | Medical consult | |
| Limited activity | Modified office care | |
| Not debilitating | ||
| IV | Debilitating systemic conditions | Emergency care |
| Constant threat to life | Medical consult | |
| Care in a hospital environment | ||
| V | Morbid patient | Maintain basic life support |
| Not expected to live |
Source: Adapted from Anesthesiology 1963;24:111.
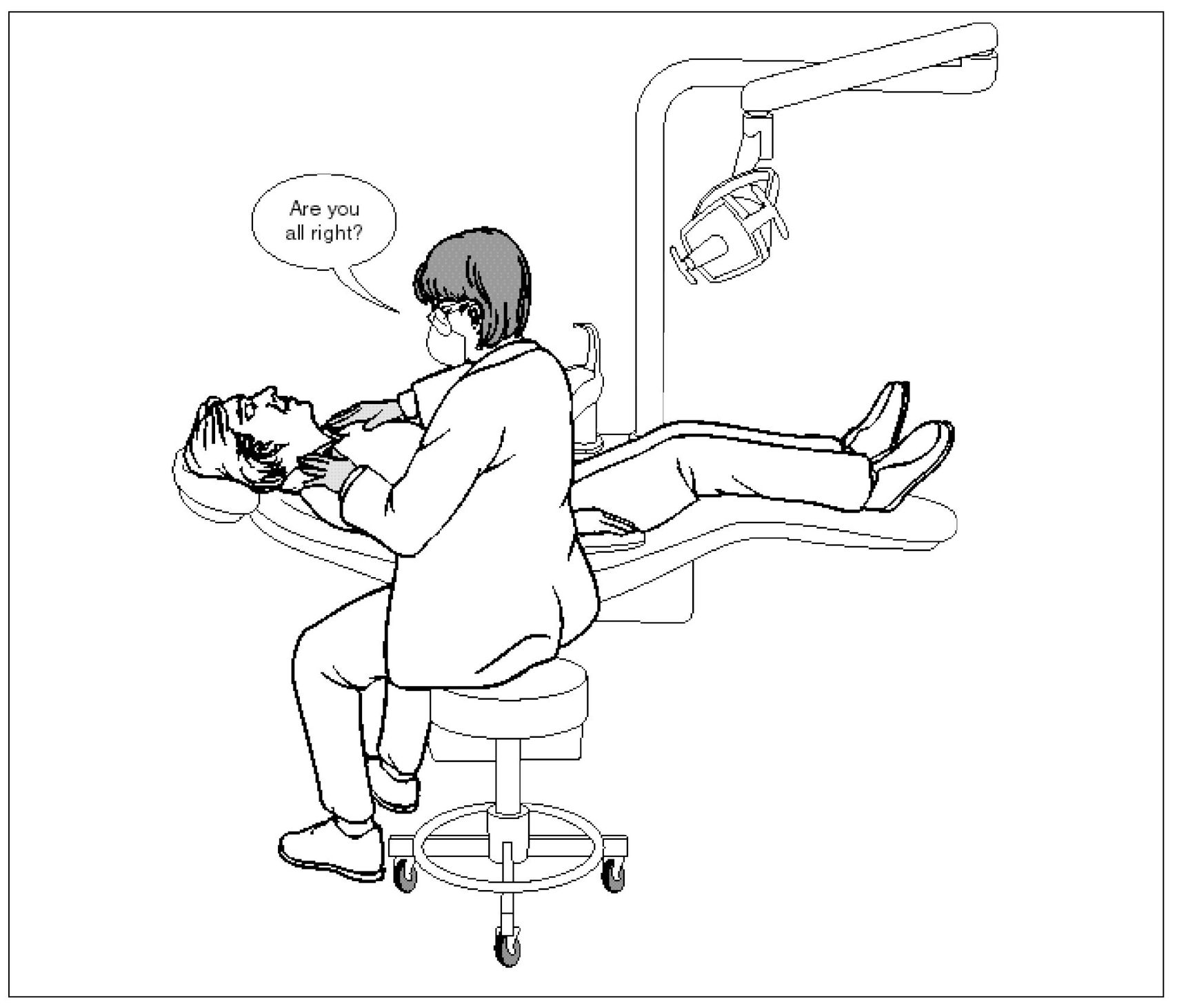
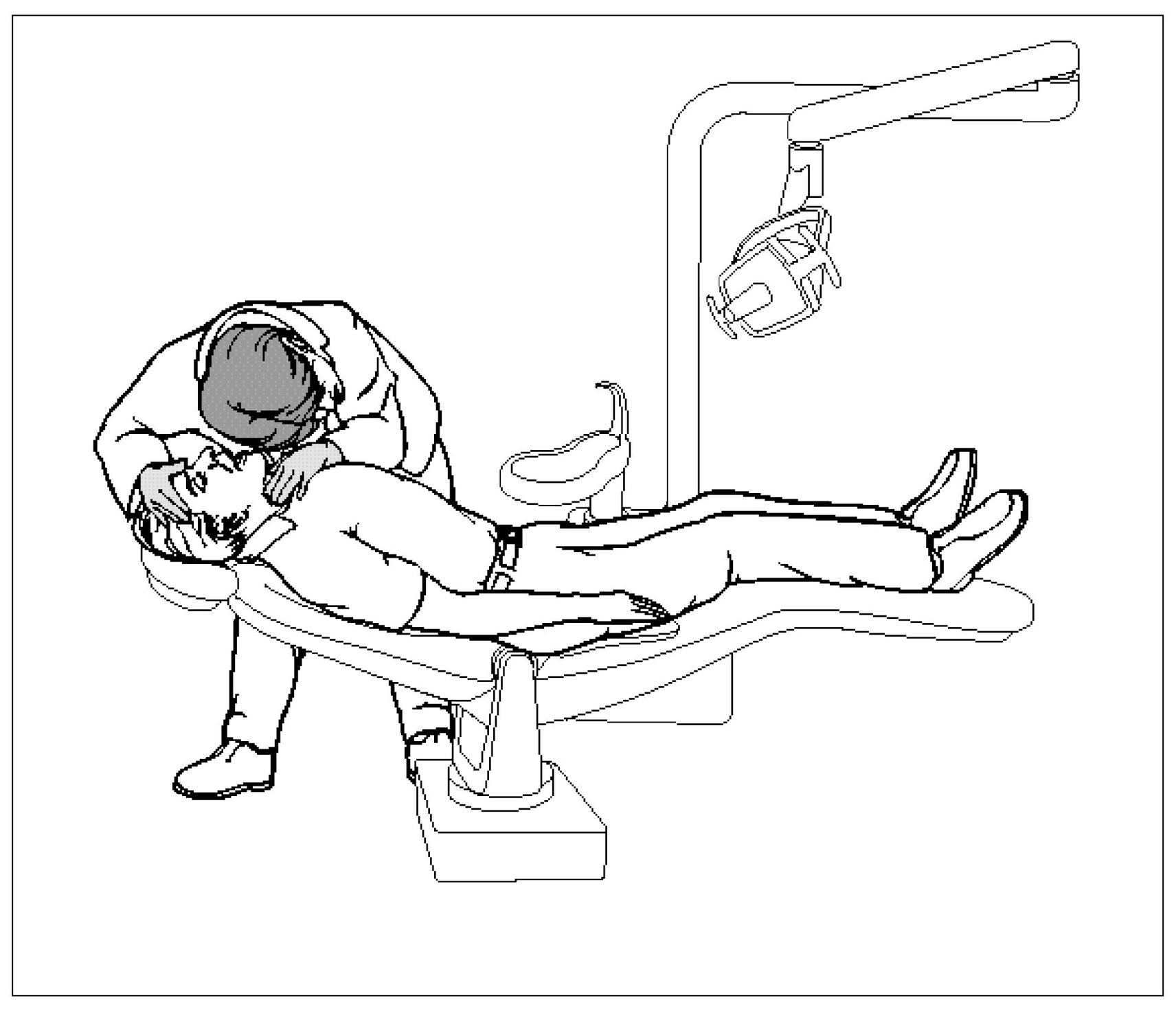
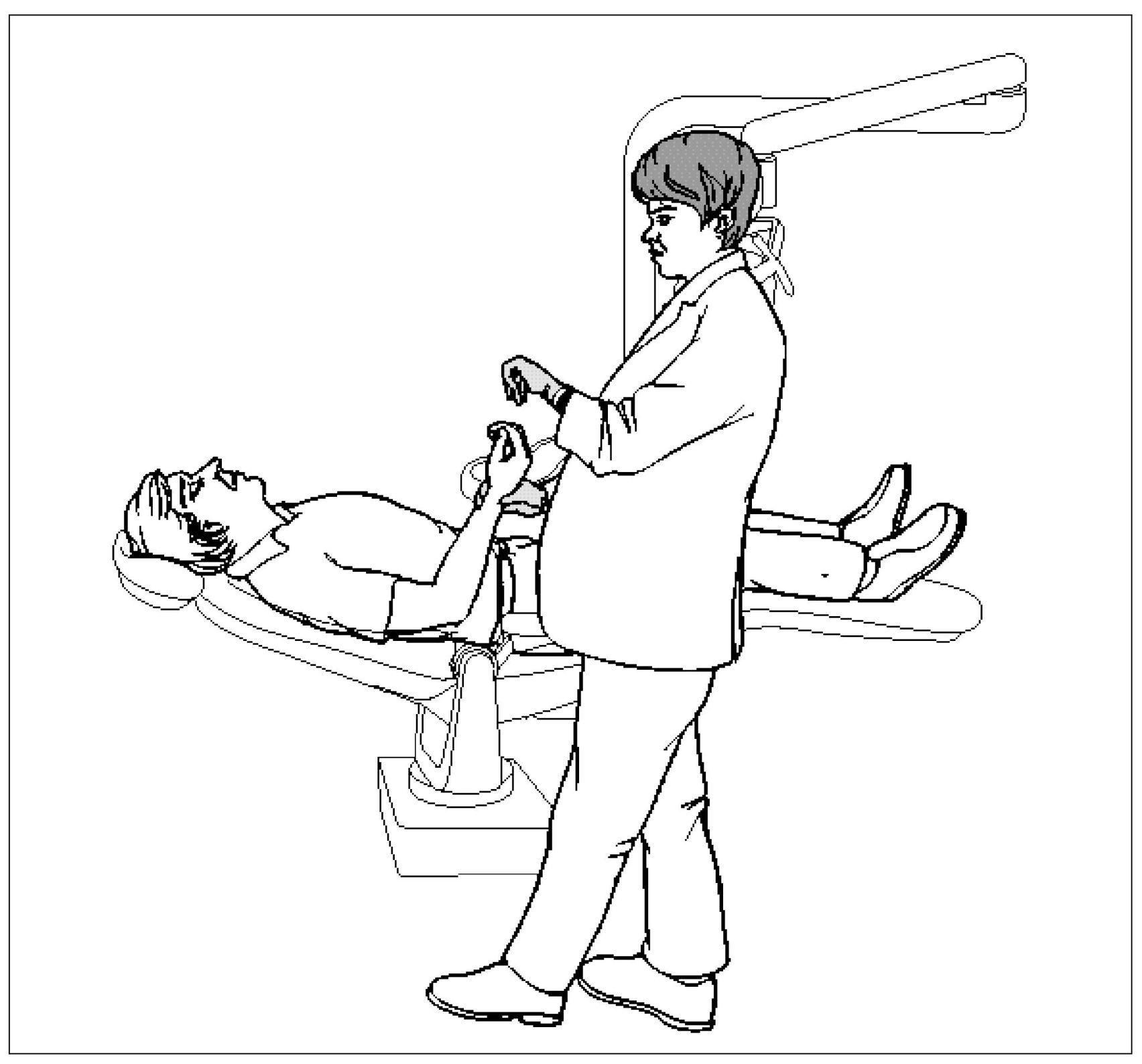
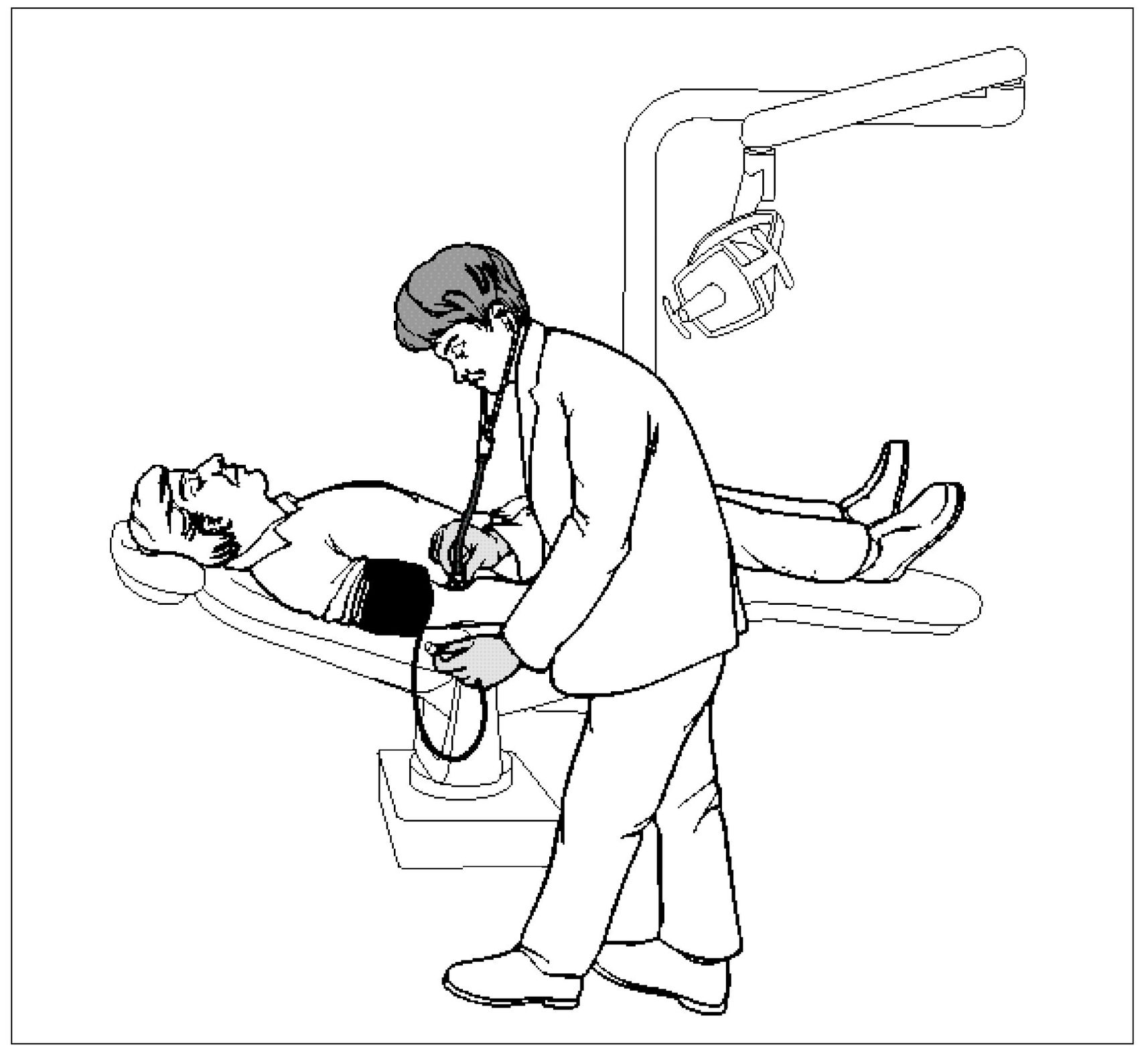
Vasovagal Syncope (Fainting)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


