Individualized Orthodontic Treatment Planning
Flavio Andres Uribe, Taranpreet K. Chandhoke, Ravindra Nanda
A well-executed, individualized treatment plan is one of the most fundamental components of orthodontic treatment. Treatment planning begins with optimal diagnosis and sequential categorization of the identified problems in order of importance. From the problem list, specific treatment objectives are generated to address each identified problem. Greater priority is given to problems that appear to be more severe or for which earlier intervention is required. Also, a patient’s chief complaint should be given high priority.
The treatment planning sequence should closely follow diagnostic findings (see Chapter 1) in the anteroposterior, transverse, and vertical dimensions. Although these dimensions have direct and indirect relationships to each other, each is analyzed separately in the problem list. In addition to problems in these three dimensions, any remarkable dental and medical findings and alignment issues are listed.
The most common medical and dental findings to be considered during orthodontic treatment are discussed in Chapter 1. The patient’s medical history should be reviewed and any systemic disease or medical condition that may have an impact on the treatment plan should be included in the problem list. Not only may these conditions affect the course of orthodontic treatment, but orthodontic treatment may have detrimental effects on existing medical and dental problems and therefore these should be reviewed carefully. Furthermore, the effect of some medications on orthodontic treatment should be explored.1,2
Significant dental problems can have a direct impact on treatment planning. An example can be seen in a patient with extensive decay in the first molars. A decision between extracting or restoring these teeth has to be made not only from a purely orthodontic perspective, but also in conjunction with other factors, such as cost–benefit and long-term prognosis.
Treatment Objectives
The cornerstone of treatment planning is the treatment objectives. These can be visualized easily in three dimensions by means of a visualized treatment objective (VTO) and an occlusogram, which will be discussed later.3
Treatment objectives can be divided into general and specific treatment objectives. These categories are related but distinct as far as determination of treatment goals is concerned. General treatment objectives are those that can be applied to any orthodontic patient regardless of his or her malocclusion. These objectives include most of the characteristics of an ideal occlusion, such as Class I occlusion (canine), normal overjet and overbite, coincident midlines, slight curve of Spee, arch width coordination, and absence of crowding, spacing, rotations, and marginal ridge discrepancies.4 These objectives do not provide the clinician with any specific information on how they are to be achieved. For example, an ideal overjet can be obtained in a Class II patient by retracting the upper incisors, flaring the lower incisors, or a combination of the two. Moreover, the nature of the incisor movement can be translation, controlled tipping, or uncontrolled tipping. If the specific objectives are not established, the clinician can choose any variety of methods, such as different appliances (Herbst, headgear, pendex, Twin Force bite corrector, elastics, bionator) or any therapy (extraction, nonextraction, surgery, implants) for Class II correction, since the only known objective is overjet reduction. A very wise phrase applies here: “If you don’t know where you are going, it doesn’t matter which road you take.”5
To provide an individualized treatment plan, specific treatment objectives must be determined.6 The general treatment objectives allow the orthodontist to communicate with the patient and guardian, while the specific treatment objectives act as a template (blueprint) for the desired treatment outcome.
Specific Treatment Objectives
Seven specific treatment objectives guide the clinician to achieve the desired outcome in the three planes of space: skeletofacial, soft tissue, occlusal plane, arch width, midlines, anteroposterior position of the incisors and molars, and vertical position of the incisors and molars.4
Skeletofacial Objectives
These objectives rely on understanding the growth status of the patient and often on the ability to predict the amount, direction, and rate of remaining growth. Due to the great variability in growth, it is difficult to define specific skeletofacial objectives. Perhaps this inability to accurately predict growth is the reason why many clinicians do not believe that specific objectives can be set in treatment planning for growing patients. This is not an issue in adult patients for whom skeletal objectives can be defined adequately, although for them a similar problem is encountered in determining the soft tissue objectives (see below).
Even though there is great variability in predicting growth, this objective is important and cannot be disregarded. A good approach is to underestimate future growth in skeletal Class II patients and overestimate growth in Class III patients. In this manner any additional growth (in a Class II patient) or limited growth (in a Class III patient) relative to the prediction would be favorable. Of course this is not always easy, especially in patients with moderate-to-severe dentofacial deformities, since growth can be the deciding factor between a surgical and nonsurgical approach to treatment.
Useful growth information is best obtained with a series of lateral cephalometric radiographs taken at 6-month to 1-year intervals. These radiographs provide important information since growth patterns are usually maintained in the majority of patients.7 Unfortunately, serial cephalograms are often unavailable when a patient initially presents for treatment. Therefore an assessment of growth potential (amount of growth left in relation to puberty) and evaluation of craniofacial morphology (Bjork indicators)8 may aid in the prediction.
It is important to note, however, that even if growth cannot be modified extensively at the level of the apical bases, significant skeletofacial changes can be achieved by affecting the dentoalveolar apparatus. This is especially evident in the vertical control of the molar, where favorable skeletofacial vertical and anteroposterior changes can be obtained with carefully selected mechanics.
In a nongrowing patient, surgery can substantially affect the skeletofacial objectives. As mentioned, the specific soft tissue component here directly relates to skeletal movements and can still be difficult to predict in these cases. However, pure skeletal changes, such as reducing mandibular prognathy in a Class III patient with a mandibular setback procedure, can be estimated and visualized with a VTO.
Soft Tissue Objectives
As mentioned above, soft tissue objectives are very much related to the skeletofacial objectives. The only aspect not covered in the skeletofacial objectives is the soft tissue changes due to dentoalveolar movement. The most remarkable changes in this area relate to the lips: reduction of interlabial gap and lip protrusion or retrusion. Direct effects on the soft tissue drape are seen with dentoalveolar movement in the vertical dimension at the molar level and in the anteroposterior dimension at the incisor level.
Anteroposterior incisor movement can result in changes at the lip level, at least to some degree.9–11 Accurate prediction of soft tissue response to incisor movement is difficult. Therefore the soft tissue objectives should be set in terms of direction (more predictable) rather than magnitude of change.
Occlusal Plane Objectives
Occlusal plane objectives are often overlooked in treatment planning. Occlusal plane goals should be considered from a frontal and lateral perspective and in conjunction with skeletal and soft tissue objectives.12 In the lateral view, anterior and posterior occlusal planes should be coincident. For example, in open-bite and deep overbite patients, the anterior and posterior occlusal planes are often at different levels. When determining specific objectives for a patient, it is a good idea to predetermine the level of the occlusal plane in order to apply proper mechanics during treatment. In deep bite patients it may be desirable to intrude anterior teeth to the level of the posterior teeth or vice versa. A straight wire ligated into all brackets has no ability to selectively intrude or extrude teeth. These mechanics are not optimal; the wire rather than the clinician ultimately controls the occlusal plane objectives. Similarly, in open-bite patients placement of a straight wire can have very undesirable results. The best option in this situation may be to treat the posterior and anterior segments separately.
Specific occlusal plane objectives in the frontal view should also be determined carefully. Often a cant in the anterior occlusal plane is associated with a midline deviation. This can be treated effectively by selective ligation of an intrusion arch or use of a cantilever to rotate the anterior teeth as a whole.13
Treatment objectives should outline not only the level of the occlusal plane, but also the cant. The term level refers to a parallel vertical movement, whereas the term cant refers to angular movement of the occlusal plane. A level change can be achieved, for example, by using an anterior bite plane, which allows eruption of posterior teeth. In addition, the application of box elastics to the posterior teeth aids in the occlusal plane leveling of the buccal segments by extrusion.14 Indiscriminate use of Class II elastics for a prolonged period of time will invariably cant (steepen) the occlusal plane, whether or not this is a desired part of the treatment plan.
Arch Width Objectives
Arch width objectives relate mainly to the intercanine and inter-molar width. The lower intercanine width has been considered to be almost unalterable, as changes in this distance yield unstable results.15 Any significant increase in the mandibular intercanine width may indicate a need for long-term fixed retention.16 More leeway has been given to the alteration of the upper canine and molar width. Increasing the arch width depends largely on the occlusal and esthetic objectives.
For occlusal correction, a definitive indicator for expansion of the maxillary arch width occurs in a case with skeletal crossbite. However, from an esthetic perspective, some clinicians may expand the maxillary arch to fill the buccal corridors and approach treatment with a nonextraction, expansion treatment.
Midline Objectives
The midline is an important occlusal and esthetic objective. This topic is discussed extensively in this book. Needless to say, the facial and dental midlines should coincide. The planning of this objective becomes more elaborate when a surgical correction due to apical base midline problems is considered. In these patients the desired dental movement must be determined in conjunction with the apical base movement.17 This is illustrated in Case 3 in this chapter, wherein an apical base discrepancy exists in the absence of a dental midline discrepancy. In this case, with the maxillary osteotomy performed, the maxilla is rotated such that the apical base deviation is corrected while the dental midline position is maintained.
Anteroposterior Objectives
Incisor Objectives.
The incisor anteroposterior objectives should be planned with consideration given to the skeletofacial and soft tissue (lips) objectives.18 The final anteroposterior position is decided after taking into consideration the nasolabial angle, facial convexity, size of nose, and ethnicity.19 Anteroposterior objectives that cannot be obtained skeletally are obtained through dental compensations (camouflage). Usually the anteroposterior incisor objective is described in terms of the incisal edge (flare, maintain, or retract). The nature of the tooth movement should be described further (controlled tipping, uncontrolled tipping, or translation). If the incisal edge position is to be maintained, root correction (controlled root movement) is the other type of incisor movement in this plane.
The anteroposterior movement of the incisor depends largely on occlusion and esthetics. Arch crowding, protrusion, overbite, and overjet are some of the occlusal factors to consider. Esthetic considerations relate to lip changes (which vary greatly in magnitude) and third-order inclination of the upper incisors.20 The final position of the upper incisors, due to their esthetic importance, must be decided during treatment planning.21 This is especially the case in surgical patients, where the incisors are positioned ideally in space and the orthodontic and surgical movements are planned so that the incisor position is maintained. In adolescent patients the final upper incisor position also needs to be considered relative to the desired lower incisor position, the overjet, and the potential differential jaw growth.
Proper lower incisor inclination has been considered essential and tied to a cephalometric norm (90 to 95 degrees) by various techniques. Labial movement beyond this norm in patients with an ideal mandibular plane to the Frankfort horizontal plane (25 degrees) has been related to instability and gingival recession. Although evidence does not completely support the predisposition of recession after labial flaring,22,23 this movement has traditionally been considered undesirable.24 It may be necessary to evaluate that patient’s oral hygiene, gingival biotype, and baseline recession prior to proceeding with a treatment plan that would further flare the lower incisors.25
Molar Objectives.
The anteroposterior position of the molars greatly depends on the final position of the incisors. Once the incisor anteroposterior position is established, the molars will need to be protracted, maintained, or distalized, depending on the arch width and amount of crowding present. Incorporating growth into the planning of the anteroposterior molar position becomes somewhat challenging if growth modification is planned.
Vertical Incisor and Molar Objectives
As mentioned above, the final vertical position of the upper and lower incisors is influenced by the occlusion (overbite) and esthetics (incisor display). The vertical incisor position, together with the anteroposterior position, are good starting reference points for treatment planning. The vertical position of the incisors can be easily defined by boundaries determined by the incisor display and overbite.
The influence of the molar vertical position on the skeletofacial objectives makes these teeth a key factor in the vertical and anteroposterior dimensions. The molars can be held against growth (relative intrusion) or absolutely intruded with the use of implants. They can also be extruded for overbite correction, although the long-term stability of this type of extrusion in adults is questionable. Furthermore, extrusion of molars should be considered carefully due to the resultant clockwise rotation of the mandible, which may negate any positive changes that occur during adolescent mandibular growth.
Dynamics of Treatment Planning
It must be emphasized that treatment plans and specific objectives are not static.26 Due to the difficulty in accurate prediction of remaining growth, an undesirable outcome may be encountered during orthodontic treatment. Moreover, the biological response to the mechanical stimulus may also be unfavorable. It should be determined whether the undesirable outcome resulted from poor mechanics or unfavorable growth, or both. Ultimately, the treatment objectives should be adjusted after a reevaluation of the new clinical situation.
Occlusogram, Visualized Treatment Objective, and 3D Virtual Planning
Two classic tools for visualizing the treatment plan are the occlusogram and the visualized treatment objective (VTO). With the advent of computers, these two procedures have become less cumbersome to perform.27 The occlusogram is a two-dimensional (2D) analysis of what would be considered a diagnostic wax setup.28 Since it is done on either a piece of paper or a screen, it allows visualization of the original problem in comparison to the desired dental and skeletofacial corrections. Through the anteroposterior dimension, the occlusogram and VTO are related to each other, generating the three-dimensional (3D) visual goals of treatment.29
The advent of cone beam computed tomography (CBCT)-derived 3D planning extends the virtual planning capabilities for the clinician, providing an even more thorough analysis of the skeletal, dental, and soft tissue components to accurately determine the specific objectives of treatment. This is particularly valuable in surgical cases and in those that involve dentofacial deformities.30–32 In addition, the digitally rendered 3D plan can be directly used for the fabrication of surgical splints without the use of conventional model surgery.
Case Reports
Three cases are presented to illustrate different diagnosis and treatment planning strategies.
 Case Report 1
Case Report 1
Patient Profile (Figs. 2-1 and 2-2)
• 17.10-year-old postpubertal female.
• Chief complaint: “My front teeth stick out and I want them straight.”

Figure 2-1 Case 1. A, Extraoral frontal view. Ovoid facial form; slight mentalis strain upon closure; no apparent pathology; interlabial gap 3.0 mm; 20% incisor display at rest clinically; midline—no major asymmetries; transverse fifths—normal intercommissural width at rest; vertical thirds—normal; mentolabial fold visible from this view. B, Extraoral smile. Incisor display on smile 90%; excessive mandibular incisor show; midlines: maxillary—0.5 mm right of facial, mandibular—on with facial; narrow smile. C, Extraoral profile. Convex soft tissue profile; protrusive upper lip; retrusive lower lip; lower facial height: throat depth within normal limits (WNL). D, Intraoral frontal view. Maxillary midline 0.5 mm to right of facial; mandibular midline on with facial; 40% overbite; good oral hygiene; slightly thin gingival biotype in lower incisor region. Intraoral right (E) and left (F) buccal views. Class II molar and canine (more severe on left); 7 mm overjet; protrusive maxillary and mandibular incisors. G, Intraoral maxillary occlusal view. 7–7 present with supernumerary teeth adjacent to molars; U-shaped arch; moderate crowding (5 mm); no caries present with some staining of pits and fissures. H, Intraoral mandibular occlusal view. 7–7 present; U-shaped arch; mild crowding (3 mm); small occlusal composites on lower 6s and staining of pits and fissures.

Medical History
Dental History
Psychosocial Profile
Enthusiastic about receiving orthodontic treatment.
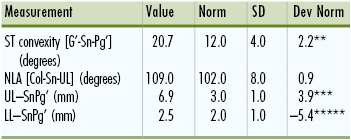
Cephalometric Summary (Fig. 2-3 and Tables 2-1 to 2-4)
Class II skeletal relationship with convex skeletal profile including:

TABLE 2-1
Case 1: Cranial Base Analysis
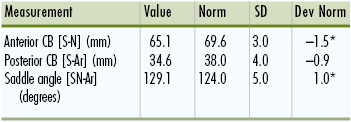
CB, cranial base; Dev Norm, deviation norm; SD, standard deviation. * indicates number of SD from norm values.
TABLE 2-2
Case 1: Maxilla-Mandible to Cranial Base Analysis
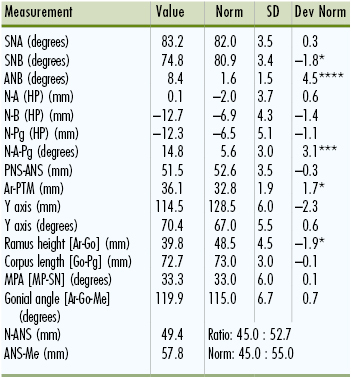
ANB, A point nasion B point; ANS, anterior nasal spine; Dev Norm, deviation norm; HP, horizontal plane; MPA, mandibular plane angle; PNS, posterior nasal spine; PTM, pterygomaxillary point; SD, standard deviation; SNA, sella-nasion A point; SNB, sella-nasion B point. * indicates number of SD from norm values.
TABLE 2-3
Case 1: Dentition
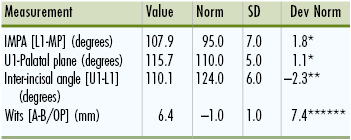
Dev Norm, Deviation norm; IMPA, incisor-mandibular plane angle; SD, standard deviation. * indicates number of SD from norm values.
Problem List
1. Medical and dental findings of significance:
• Supernumerary teeth adjacent to maxillary first molars
• Small occlusal composite restorations on posterior dentition
• Thin gingival biotype in lower incisor region
• Skeletal: Class II and convex skeletal profile due to retrognathic mandible
• Skeletal: Slightly short ramus height, vertical thirds within normal limits
4. Transverse:
• Skeletal: Normal skeletal transverse dimensions
5. Alignment:
• Maxillary arch: moderate (5-mm) crowding
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


