Diagnosis and Treatment Planning for Single Implants
Etiology and Treatment of Tooth Loss
Indications for Root Canal Treatment and Restoration
Systemic and Local Health Factors
Patient Comfort and Perceptions
Biologic Environmental Considerations
Extraction Without Tooth Replacement
Tooth Extraction and Replacement with a Fixed Partial Denture
At the conclusion of this chapter, the reader will be able to:
 . Discuss the etiologies of tooth loss and their treatments.
. Discuss the etiologies of tooth loss and their treatments.
 . List the indications for and contraindications to root canal treatment.
. List the indications for and contraindications to root canal treatment.
 . Identify factors affecting planning for root canal treatment.
. Identify factors affecting planning for root canal treatment.
 . Discuss the consequences of tooth loss without replacement.
. Discuss the consequences of tooth loss without replacement.
 . Discuss the effect of implants on prosthodontics.
. Discuss the effect of implants on prosthodontics.
 . Discuss the indications for a single implant.
. Discuss the indications for a single implant.
 . Identify factors affecting treatment planning for a single implant.
. Identify factors affecting treatment planning for a single implant.
Attempts were made to use dental implants in ancient civilizations, and as early as the 1800s endosseous root form implants were placed. In the twentieth century, implants were used in completely and partially edentulous patients to provide much-needed stability and function for fixed and removable prostheses (Figure 2-1). However, implant survival rates were not as high as desired, and sometimes substantial bone loss occurred in conjunction with loss of the implant. The survival rates of implants improved substantially with the introduction of modern cylindrical endosseous implants,1,2 adding another valuable treatment option for teeth that could not be retained endodontically or periodontally (Figure 2-2).

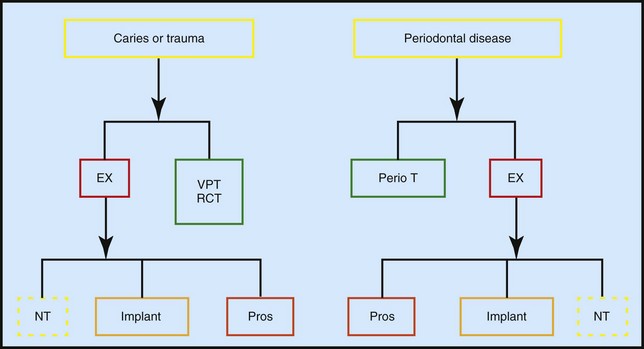
By conducting a systematic examination and careful analysis of the data obtained, the clinician is better equipped to make the right diagnosis. Once the diagnosis has been made, appropriate treatment planning can be carried out for most patients (Figure 2-3). However, treatment planning can become quite complicated when the expectations of the involved parties (patients, insurance companies, and dentists) are not completely met. An ideal treatment plan addresses the chief complaint of the patient, provides the longest lasting, most cost-effective treatment, and meets the patient’s expectations. In this way, treatment planning is truly a patient-centered process. Adequate treatment planning also includes relevant scientific evidence and preserves the biologic environment while maintaining or restoring esthetics, comfort, and function.
Etiology and Treatment of Tooth Loss
Although the main causes of tooth loss are decay and periodontal disease, traumatic injuries can also result in significant tooth loss. The extent of damage to a tooth as a result of these injuries depends on the force of impact. Enamel fractures, crown fractures without pulp exposure, crown fractures with pulp exposure, crown-root fractures, root fractures, tooth luxations (concussion, subluxation, lateral luxation, extrusive luxation, intrusive luxation), avulsions, resorptions, and alveolar fractures are all potential outcomes of such trauma.3 Because of the range of injuries, clinicians should be prepared to treat affected teeth with a variety of procedures, ranging from enamel recontouring and smoothing of rough edges to replantation of an avulsed tooth.3
Regardless of the specific nature of the trauma, it is important to note more generally that trauma to teeth affects the dental pulp either directly or indirectly. Endodontic considerations, therefore, are vital in the evaluation and treatment of dental injuries. In crown fractures with pulp exposure or crown-root fractures, the pulpal status and the degree of root development (Figure 2-4) are the major factors in treatment planning.4 If the diagnosis is reversible pulpitis, the treatment of choice is vital pulp therapy, regardless of the degree of root development. If the diagnosis is irreversible pulpitis or pulpal necrosis, the amount of root development determines the treatment.4 If the apex is closed, root canal therapy can be performed, with high survival rates.5,6 Teeth with irreversible pulpitis, pulpal necrosis, or immature apices present additional challenges to clinicians during obturation should endodontic treatments be required.
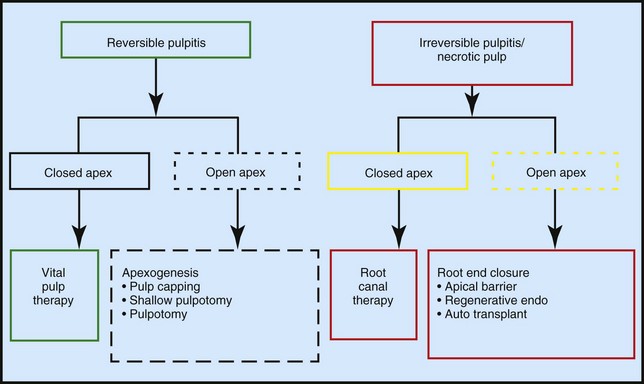
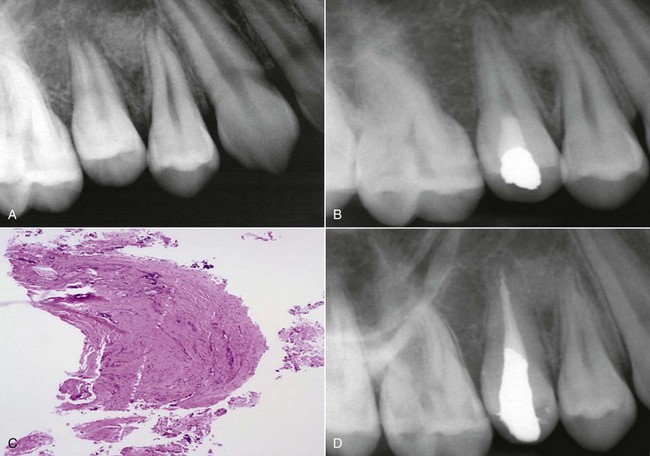
Conventionally, the apexification procedure carried out during such treatments consists of multiple long-term applications of calcium hydroxide to create an apical barrier before obturation of root canals.7 Because this procedure might alter the mechanical properties of dentin and make the teeth more susceptible to root fractures,8 a one- or two-step artificial apical barrier using mineral trioxide aggregate (MTA) has been suggested.7 High success rates have been reported for this procedure (Figure 2-5).9 However, the procedure may not result in complete root formation and may not reduce the chance of root fracture.7
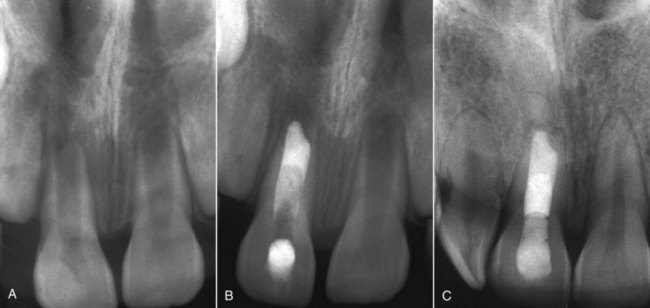
The ideal outcome for a tooth with an immature root or a necrotic pulp is regeneration of pulp tissue into a canal capable of promoting continuation of normal root development.10 A growing body of evidence suggests that regeneration of the pulp, along with continued growth of the root, may in fact be possible after pulpal necrosis and the development of apical pathosis in teeth with immature apices (Figure 2-6). Several single patient treatment reports and treatment series have been published demonstrating radiographic signs of continued thickening of the dentinal walls and subsequent apical closure of roots in teeth with necrotic pulps, open apices, and periapical lesions.10
Luxation injuries involve trauma to the supporting structures of the teeth and often affect the neural and vascular supply to the pulp.3 Every effort should be made to preserve the natural dentition in these cases. If that is unsuccessful, alternative treatments include removable partial dentures, fixed partial dentures, autotransplantation, and single implants.
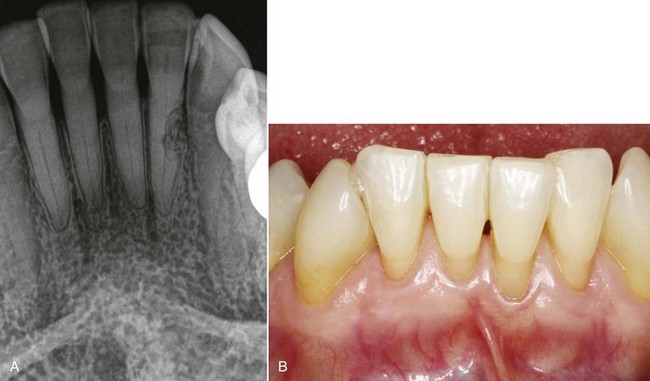
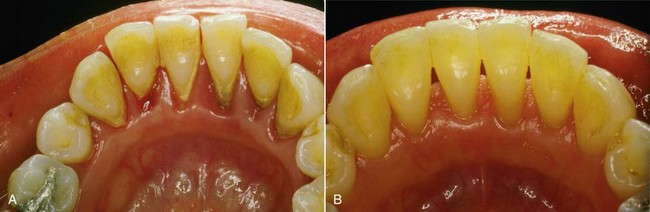
Another major cause of tooth loss is severe inflammation of the periodontium. With the establishment of extensive periodontal inflammation, teeth start to shift position, and in severe cases they may be lost (Figure 2-7). Extrusion or protrusion of maxillary incisors after periodontal bone loss, destruction of papillae, or loss of maxillary or mandibular anterior teeth may seriously damage facial expression.
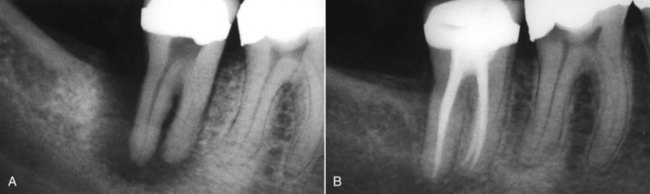
Traditionally, all efforts were made to save teeth with periodontal disease (Figure 2-8). Currently, the high survival rates of implants have affected the popularity of this approach, causing a paradigm shift in periodontics.11 The benefits of successful treatment of a tooth with periodontal disease include (1) conservation of the crown and root structure, (2) preservation of alveolar bone and accompanying papillae, (3) preservation of pressure perception, and (4) lack of movement of the surrounding teeth. Extraction, on the other hand, can include some harmful effects, such as (1) bone resorption,12 (2) shifting of adjacent teeth,13–15 and (3) reduced esthetics and chewing ability.16

Studies on the long-term prognosis for teeth with periodontal disease show less than 10% tooth loss for periodontal reasons.17–19 Single rooted teeth have a better prognosis than do molar teeth.17–19 Cases with furcation involvement, with or without surgical intervention, are associated with a poorer prognosis than are cases without furcation involvement.
Recent innovations in implant dentistry have also reduced the reliance on higher risk periodontal procedures for tissue preservation and regeneration in teeth with moderate to severe periodontal disease.22 Surveys conducted by the American Academy of Periodontology in 2004 showed that 63% of periodontists put primary emphasis on periodontics, and 27% put primary emphasis on implants.23
Although periodontal disease affects many teeth, the major cause of tooth loss is dental decay. Microorganisms in dental caries are the main source of irritation to the dental pulp and periradicular tissues.24 As the decay progresses toward the pulp, the intensity and character of the infiltrate change. As a consequence of exposure to the oral cavity and caries, the pulp harbors bacteria and their byproducts. The dental pulp usually cannot eliminate these damaging irritants. At best, defenses temporarily impede the spread of infection and tissue destruction.
If irritation persists, the ensuing damage becomes extensive and spreads throughout the pulp. As a consequence of pulpal necrosis, pathologic changes can occur in the periradicular tissues, resulting in the development of periapical lesions (Figure 2-9). Periapical lesions have been classified into five main groups: (1) symptomatic (acute) apical periodontitis, (2) asymptomatic (chronic) apical periodontitis, (3) condensing osteitis, (4) acute apical abscess, and (5) chronic apical abscess.24
Indications for Root Canal Treatment and Restoration
Indications for root canal treatment include teeth with irreversible pulpitis; necrotic pulps, with or without periapical lesions that have restorable crowns; treatable periodontal conditions; salvageable resorptive defects; and favorable crown-to-root ratios.25 Teeth with pulpal and periapical pathosis that have a restorable crown, sound periodontal structures, an adequate crown-to-root ratio, and no major tooth resorption must be saved by root canal treatment. When such posterior teeth are saved and are extensively restored or are missing considerable coronal tooth structure, crowns are indicated. In a comparative study, Aquilino and Caplan26 found a strong association between crown placement and the survival of endodontically treated teeth. In addition, a retained tooth may be at risk of future root fracture and development of caries or periodontal disease. These factors should be considered during treatment planning.
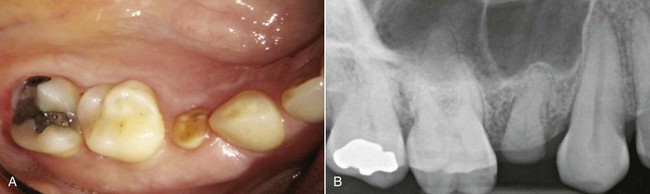
Root canal treatment is contraindicated or results in less than optimal tooth fracture resistance when limited tooth structure remains and the overlying crown cannot engage at least 1.5 to 2 mm of tooth structure with a cervical ferrule (Figure 2-10).27,28 When a post is required in a root canal–treated tooth to retain the core, the tooth is weakened but the negative effect of the post is countered by a 2-mm ferrule. When a fixed partial denture is attached to root canal–treated teeth, the teeth fail more often than do teeth with vital pulps29–31; this emphasizes the need to exercise caution with longer span prostheses and heavier occlusal forces, as indicated by substantial wear facets.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


