The Relevance of Scientific Evidence in the Decision-Making Process
Treatment Outcomes in Single Implant Therapy
At the conclusion of this chapter, the reader will be able to:
 . Understand the clinical performance of single implant therapy based on current scientific evidence.
. Understand the clinical performance of single implant therapy based on current scientific evidence.
 . Analyze and compare single implant restoration to other alternatives from both a patient perception and psychosocial point of view.
. Analyze and compare single implant restoration to other alternatives from both a patient perception and psychosocial point of view.
 . Learn the incidence of the most prevalent complications associated with single implant therapy as they have been reported in scientific literature.
. Learn the incidence of the most prevalent complications associated with single implant therapy as they have been reported in scientific literature.
 . To understand the expected esthetic outcomes of a single tooth replacement by means of a dental implant.
. To understand the expected esthetic outcomes of a single tooth replacement by means of a dental implant.
Over the past 30 years, the insertion of dental implants to restore function and esthetics in patients who are completely or partially edentulous has become a well-documented surgical and prosthetic procedure.1–5 Single missing or failing teeth are commonly replaced with dental implants, both anteriorly and posteriorly, and the process has been studied extensively. Experimental studies and clinical trials have provided ample information on design, clinical procedures, survival and failure rates, and complications.
The term evidence based means the deliberate use of current evidence as a guide in treatment, recognizing that no study is perfectly designed in every aspect or applicable to every patient.6
The use of older studies, which may have involved techniques and materials that differ significantly from current practice, must be considered with great caution. Today’s restorative dentist has a greater number of options for tooth preparation techniques7,8 and a greater selection of restorative materials.9–11 The field of implant therapy has evolved at least as quickly as that of restorative dentistry in general. A wider variety of implant diameters, lengths, and morphologies is available, and implant surface technology12,14,15 and improvements in macrodesign12–15 have dramatically altered many of the basic principles of dental implantology. The time necessary to obtain osseointegration has been significantly reduced,12 and the initial osteointegrated interface has been strengthened.12,14,15
Clinical Outcomes
Based on the high success rates achieved with implants placed as described by Brånemark et al. for the restoration of edentulous and partially edentulous arches,16 some thought that single tooth replacement by a dental implant could overcome the limitations observed in classic prosthodontic therapies.17–19 Outcomes of this technique have been evaluated using various survival and success criteria,20–24 but the criteria elaborated by Albrektsson et al.20 are probably the most commonly used in dental implant literature. These researchers defined a successful implant as one that:
 Remains immobile when tested individually
Remains immobile when tested individually
 Does not demonstrate any evidence of peri-implant radiolucency under radiographic examination
Does not demonstrate any evidence of peri-implant radiolucency under radiographic examination
 Shows a vertical bone loss of less than 0.2 mm annually after the implant’s first year of service
Shows a vertical bone loss of less than 0.2 mm annually after the implant’s first year of service
 Does not have persistent or irreversible signs and symptoms (e.g., pain, infection, or neuropathies)
Does not have persistent or irreversible signs and symptoms (e.g., pain, infection, or neuropathies)

The Albrektsson criteria were developed at a time when determining the biologic outcomes of titanium implants was important to prove their higher reliability over alternatives made of other materials. Initially, restorative and patient-based parameters received less attention. Mechanical and esthetic parameters were later evaluated,25–27 as practitioners’ demands for greater predictability and natural-looking restorations increased. However, criteria that analyze a wider number of parameters are far from being established as performance indicators in dental implant literature.
Delayed Implant Placement
Traditionally dental implants were placed according to a two-stage protocol.16 Implants were submerged beneath the soft tissues and allowed to heal undisturbed. Research findings indicated that primary implant stability and lack of micromovement were necessary to achieve predictable levels of osseointegration.28,29
Some thought that if movement occurred, the healing process would be altered and the implant would be encapsulated by soft tissues30 instead of anchored in bone. With a two-stage approach, the risk of transmitting undesirable loads to the healing bone at the implant interface was reduced.
Subsequently a one-stage protocol was developed.31 With this approach, flaps were repositioned and sutured around the supraosseous neck of the implant (single-stage implant) or around a healing abutment (two-stage implants placed in a one-stage protocol), which eliminated the need for a second surgical intervention to expose the implant connection. Success and/or survival rates for this modality ranged from 95.4% to 99.1%.32–34
In a recent report in the Cochrane Database Systematic Review, Esposito et al.35 found no statistically significant differences between the two protocols. However, the data suggested that fewer implant failures occurred with the two-stage approach, especially in completely edentulous patients. These authors hypothesized that a one-stage approach might be preferable in partially edentulous patients, because it eliminates one surgical intervention and shortens the treatment time. A two-stage approach was proposed in certain specific situations, such as when (1) an implant has not obtained optimal primary stability; (2) barriers are used for guided tissue regeneration; and (3) removable provisional prostheses might transmit excessive forces to the exposed abutments, especially in fully edentulous patients.
A systematic review by Den Hartog et al.36 in 2008 found an overall implant survival rate of 92.8% when data were pooled from 11 studies following 248 implants during an average follow-up period of 2.8 years. The review combined data from implants placed in one-stage and two-stage protocols.
Immediate Implant Placement
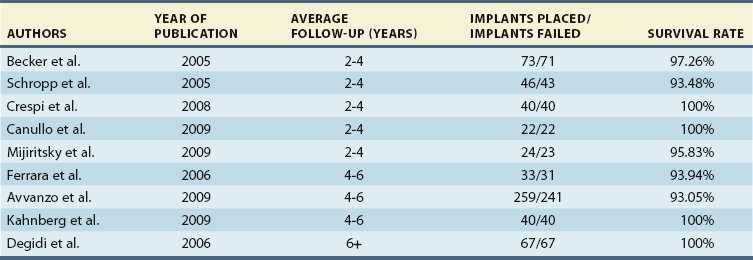
Clinical studies report data on the number of implants placed and lost over a specified time. In the combined data extracted from several studies37–45 with a minimum follow-up time of 2 years, published on single immediate implants up to 2009, 604 implants were placed and were observed for 2 to 10 years. Twenty-six implants were lost (mean implant loss rate of 4.3%). For illustrative purposes, the studies were categorized into three groups (Table 11-1). In the first group37–41 (follow-up period of 2 to 4 years), an overall survival rate of 97.08% was observed. In the second group42–44 (follow-up period of 4 to 6 years), a survival rate of 93.98% was observed. Surprisingly, in the third group45 (minimum sample follow-up of 6 years), a slightly higher survival rate was observed; the survival rate was 100% after the study period.
Complications
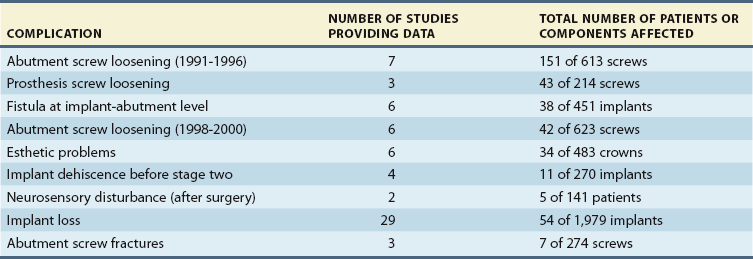
The information on success, failure, and complications presented in the following sections was developed by combining the raw data from clinical studies that evaluated implant single crowns. A mean was calculated for each type of complication by combining the data from each study. The purpose of the information is to suggest clinical trends rather than provide statistically valid incidence data. Table 11-2 identifies the types of complications that have been encountered in the clinical studies and provides a mean based on the number of studies that provided raw data related to that complication.
Implant Loss
In the combined data from single implant studies,46–66 1,979 implants were placed and were observed for 1 to 10 years; 54 implants were lost (mean implant loss rate of 3%). This failure rate, shared with implants that support mandibular fixed complete dentures, is the lowest failure rate encountered in implant prosthodontics. Three studies60,70,72 provided data that permit a comparison of maxillary and mandibular implant loss. Six studies* provided data on the time when the implants were lost; 47% of the implants were lost preprosthetically, and 53% were lost postprosthetically.
Other Complications
Other single implant complications identified in the studies included abutment screw loosening with early screw designs reported from 1991 to 1996 (25%)†; prosthesis screw loosening (20%)56,65,74; fistulas at the implant abutment level (8%)‡; abutment screw loosening with newer screw designs reported from 1998 to 2000 (7%)61,62,66,67–69; esthetic problems (7%)§; implant dehiscence before stage two (4%)46,53,58,59; neurosensory disturbances after surgery (4%)46,58; and abutment screw fracture (2%).58,66
Psychosocial Outcomes
The psychosocial effects of single implant treatment have been described in scientific studies. Patient satisfaction and pain perception have been studied in the dental implant literature. However, studies focusing on those two parameters in relation to single implant replacement therapies are scarce. Interestingly, fewer than 2% of publications on dental implants deal with patient-centered issues.76
Few studies have evaluated patient satisfaction in single implant restorations. In a recent study by Vermylen et al.,77 a sample of 48 patients (52 implants) was studied after treatment with single implant restoration. The patients in this study were mailed a post-treatment questionnaire requesting information on their satisfaction with the treatment provided. The study observed that the patient opinion on the treatment was positive. Although all the patients were positive in recommending the treatment to others, almost a quarter of them responded negatively when asked whether they would be willing to undergo a similar treatment again. The authors of this study hypothesized that this result was probably related to the time elapsed between implant placement and cementing of the restoration, describing this issue as the major disadvantage perceived by patients. Other studies have shown that a one-stage surgical procedure may reduce healing time and enhance patient acceptance.78
Similar results were observed in a later study by Bacarat et al.79 In this study, patient expectations before treatment and satisfaction after treatment were rated on a visual analog scale and correlated; the satisfaction value was about 40% higher than the expectations value. The results of this study confirm that single tooth replacement is a very satisfactory procedure that may surpass patients’ expectations.
Pain may be defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage.80 Given the surgical nature of the dental implant procedure, different degrees of pain in relation to the extent of the procedure can be expected. Limited published data are available on the pain associated with the surgical placement of dental implants80,81 or on factors associated with such pain.82 These authors know of no study that has evaluated pain perception in single implant therapy. However, some studies have reported a significant association between the number of implants placed and pain during the surgery.74 In a study by Al-Khabbaz et al.,83 patients with multiple implants were found to be 1.3 times more likely to experience pain during surgery than those who received a single implant. In the same study, the mean postoperative pain scores were highest 24 hours after surgery and decreased gradually after 1 week. With regard to the intensity of the reported pain, most patients reported mild pain (69.7% after 24 hours, 56.5% after 1 week, and 5.1% after 6 weeks), and a few patients reported moderate or severe pain (10.6% after 24 hours, 3.8% after 1 week, and none after 6 weeks). In general, studies have shown that maximum pain levels appear 6 to 24 hours after implant placement, and most patients rate pain as mild.80,81 Factors associated with pain perception are listed in Table 11-3.
Table 11-3
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


