CHAPTER 19. Common benign mucosal swellings
FIBROUS POLYPS, EPULIDES AND DENTURE-INDUCED GRANULOMAS → Summary p. 323
Fibrous nodules are the most common soft-tissue swellings of the mouth. They are not neoplasms but hyperplastic swellings that develop in sites subject to chronic minor injury and/or low-grade infection (Box 19.1). Fibromas are not recognised as an entity and, in any case, cannot be distinguished from fibrous hyperplasia. The term epulis (literally, ‘on the gingiva’) refers only to the site. It has no implications for the cause or histology but, in practice, most epulides are fibrous.
Box 19.1
Fibrous nodules: practical points
• The most common oral tumour-like swellings
• Most frequently form at gingival margins (fibrous epulis) or in relation to a denture
• They are hyperplastic responses to chronic irritation
• Should be excised complete and sent for histological examination
Irritation of the gingival margin by the sharp edge of a carious cavity or by calculus may lead to the formation of a fibrous epulis; irritation of alveolar or palatal mucosa by a rough area on a denture may provoke development of a denture granuloma. Though different names are given to these lesions they are similar in origin and structure.
Clinical features
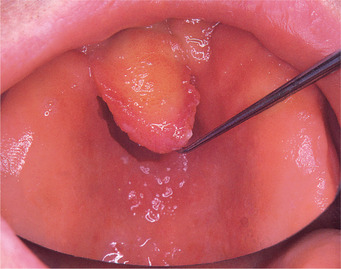
A fibrous epulis is most common near the front of the mouth on the gingiva between two teeth (Fig. 19.1). Fibrous polyps can also form on the buccal mucosa (Fig. 19.2). Denture-induced hyperplasias (‘denture granulomas’) often form at the edge of dentures (Fig. 19.3). These swellings are pale and firm but may be abraded and ulcerated, and then inflamed.
 |
| Fig. 19.1
Fibrous epulis. This lesion, arising from the gingival margin between the lower central incisors, is firm, pink and not ulcerated.
|
 |
| Fig. 19.2
Fibrous polyp. This lesion on the buccal mucosa has arisen as a result of cheek biting and is a firm, painless polyp covered by mucosa of normal appearance.
|
 |
| Fig. 19.3
Denture-induced granuloma. Fibrous hyperplasia at the posterior border of this upper partial denture has resulted in a firm mucosal swelling moulded to fit the denture.
|
‘Leaf fibroma’ is another fibrous overgrowth which forms under a denture but has become flattened against the palate (Fig. 19.4). It may be difficult to see until lifted away from its bed.
 |
| Fig. 19.4
‘Leaf fibroma’. Flat lesions formed between the denture and mucosa are often termed leaf fibromas because of their shape. Raising this example with a probe reveals its pedunculated shape.
|
Pathology
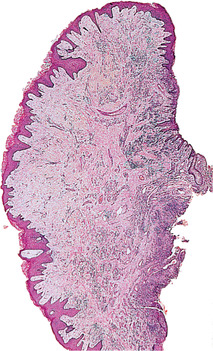
These nodules consist of irregular interlacing connective tissue fibres without encapsulation but covered by epithelium, which is usually hyperplastic (Fig. 19.5).
 |
| Fig. 19.5
Fibrous polyp. The lesion is composed of mature fibrous tissue covered by hyperplastic epithelium with spiky rete processes. A few inflammatory cells are present near the base.
|
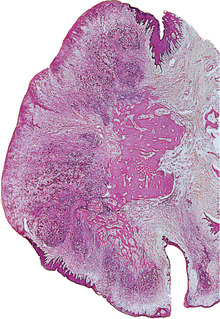
Bone formation is sometimes seen in a fibrous epulis (Fig. 19.6). In American texts, a fibrous epulis containing bone is termed (in an apparent desire to cause confusion) a ‘peripheral ossifying fibroma’, even though it has no relation to the ossifying fibroma of bone and is not a fibroma.
 |
| Fig. 19.6
Fibrous epulis with ossification. Much of the surface of this pedunculated nodule is ulcerated and hyperplastic epithelium covers the margins. Centrally, the lesion is very cellular, partly as a result of inflammatory infiltrate, and trabeculae of woven bone are being deposited and maturing into lamellar bone. The presence of bone in a fibrous epulis appears to be of no clinical significance.
|
Fibrous nodules should be excised together with the small base of normal tissue from which they arise. In the case of a fibrous epulis, the underlying bone should be curetted. There should be no recurrence if this is done thoroughly and the source of irritation is removed.
Histological examination is needed to confirm that an epulis is fibrous and not a giant-cell lesion, pyogenic granuloma or a malignant tumour, which can very rarely form on the gingival margin and simulate a non-neoplastic epulis.
Giant-cell fibroma
This variant is distinguished microscopically by large, mononucleate, stellate, darkly-staining cells (quite unlike the multinucleate cells of a giant-cell granuloma) and less conspicuous multinucleate cells, scattered between short, coarse fibrous tissue bundles. Clinically, giant-cell fibromas are typically pedunculated and usually arise from the gingivae or tip of tongue. The surface is frequently verrucous.
The treatment is the same as for a fibrous epulis.
PAPILLARY HYPERPLASIA OF THE PALATE
Nodular overgrowth of the palatal mucosa is occasionally seen, particularly under dentures in older persons in whom low-grade trauma or infection exacerbates the proliferation (Fig. 19.7). Candidosis is sometimes superimposed but is not the cause. Mild palatal papillary hyperplasia is also occasionally seen in non-denture wearers.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


