Dental caries and the assessment of restorations
Classification of caries
• Primary caries – caries developing on unrestored surfaces
• Secondary or recurrent caries – caries developing adjacent to restorations
• Residual caries – demineralized tissue left behind before filling the tooth.
Levels of disease
• D1 – Clinically detectable enamel lesions with intact surfaces
• D2 – Clinically detectable cavities limited to enamel
These distinctions are important with regard to management. Lesions at levels D1 and D2 are generally managed using preventative measures, whereas lesions at the D3 or D4 level are likely to require restorative treatment. Detection of lesions of caries and being able to assess the level of disease are therefore crucial in determining clinical treatment.
Diagnosis and detection of caries
Approximal caries
Radiographic detection of lesions of caries
Bitewing radiographic techniques, using both film packets and digital sensors (solid-state and phosphor plates) as the image receptor, were described in Chapter 8. For caries detection, film packets and phosphor plates are preferred as the imaging area of the equivalent sized solid-state sensors is smaller. It has been reported that on average three fewer interproximal tooth surfaces are shown per image.
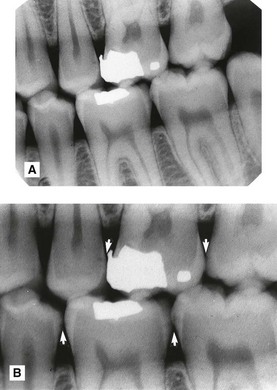
Approximal lesions of caries are detectable radiographically only when there has been 30–40% demineralization, so allowing the lesion to be differentiated from normal enamel and dentine. The importance of optimum viewing conditions for both film and digital images, as described in Chapter 16, cannot be overemphasized when looking for these early subtle changes. Magnification is of particular importance, as shown in Fig. 17.1.
Radiographic assessment of caries activity
In the UK, the 2013 Faculty of General Dental Practice (UK)’s booklet Selection Criteria for Dental Radiography recommends that the frequency of these follow-up radiographs be linked to the caries risk of the patient. There are three risk categories – high, moderate or low risk – for both children and adults. The Selection Criteria booklet contains a number of evidence-based recommendations, the main ones of which are summarised in Table 17.1. As can be seen for high risk children and adults 6-monthly time intervals are recommended, for moderate risk patients 12-monthly intervals and for low risk children 12–18 month intervals and for low risk adults 2-yearly intervals
Table 17.1
| Recommendation | Evidence-based grading* |
| All children designated as high caries risk should have six-monthly posterior bitewings taken until no new or active lesions are apparent and the individual has entered another risk category (Bitewings should not be taken more frequently and it is imperative to reassess caries risk in order to justify using this interval again.) | B |
| All children designated as moderate caries risk should have annual posterior bitewings taken until no new active lesions are apparent and the individual has entered another risk category | B |
| All children designated as low caries risk should have posterior bitewings taken at approximately 12–18 month intervals in primary dentition and at approximately two-yearly intervals in the permanent dentition. More extended radiographic recall intervals may be employed if there is explicit evidence of continuing low caries risk | B |
| All adults designated as high caries risk should have six-monthly posterior bitewings taken until no new or active lesions are apparent and the individual has entered another risk category (Bitewings should not be taken more frequently and it is imperative to reassess caries risk in order to justify using this interval again. It is also important to remember that rates of caries progress in enamel and dentine will differ and that rates in adults may well be slower than in children) | C |
| All adults designated as moderate caries risk should have annual posterior bitewings taken until no new or active lesions are apparent and the individual has entered another risk category | C |
| All adults designated as low caries risk should have posterior bitewings taken at approximately two-yearly intervals. More extended radiographic recall intervals may be employed if there is explicit evidence of continuing low caries risk. | C |
| The taking of ‘routine’ radiographs based solely on time elapsed since the last examinations is not supportable. | C |
| Intervals between subsequent radiographic examinations must be reassessed for each new period as patients can move in and out of caries risk categories over time. | C |
| CBCT should not be used as a routine method of caries diagnosis | B |
*Evidence-based grading B = based on evidence from well conducted clinical studies but with no specific in vitro validation studies; C = based on evidence from expert committee reports or opinions and/or clinical experience of respected authorities and indicates an absence of directly applicable studies of good quality.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


