16
The airway
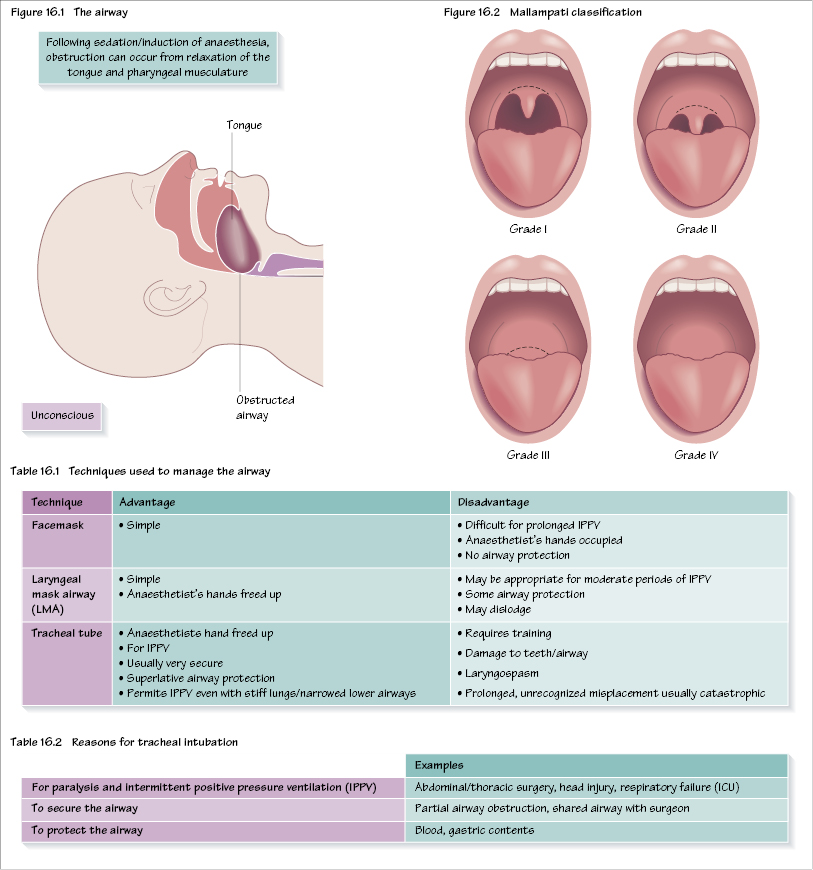
Maintaining the airway is the most fundamental aspect of clinical anaesthetic practice. Failure to do so, and the concomitant hypoxia, is still a significant cause of death from anaesthesia. No patient should receive GA or sedation without prior assessment of the airway. During anaesthesia and sedation there is muscular relaxation of the pharynx, which may lead to airway obstruction (Figure 16.1). In addition, many of the drugs used will cause respiration to cease. Ensuring adequate oxygenation is the priority at all times. Many, but not all, difficult airways may be anticipated in advance.
A separate area is that of the unstable neck, whereby manipulation of the neck may put the patient at risk of spinal cord injury.
Airway assessment
Traditionally, the gold standard of airway management is tracheal intubation, and the majority of assessments relate to the ease or difficulty of this process.
History
Ask about:
- past anaesthetic history – see old notes, Medic Alert bracelet;
- surgery/radiotherapy to head and neck;
- obstructive sleep apnoea (OSA);
- conditions affecting tongue size (e.g. acromegaly, infections, tumours);
- conditions affecting neck mobility (e.g. ankylosing spondylitis, infections, tumours);
- conditions affecting mouth opening (e.g. temporamandibular joint dysfunction).
General examination
This includes:
- Look for external signs of surgery/radiotherapy to head and neck.
- Assess the airway from in front of the patient, including: receding jaw, protruding upper incisors, large tongue, large neck, obesity.
- Tumours, infection, trauma, swelling or burns and scarring of the airway strongly suggest problems.
Tests
A number of tests exist but none are very specific or sensitive. Most attempt to predict the ease of view during subsequent laryngoscopy. These include:
- mouth opening: this should be 4–6 cm;
- Mallampati classification (Figure 16.2): on full opening of the mouth the faucial pillars, uvula and soft palate sequentially disappear; scores of 3 and 4 are associated with difficult intubation;
- forward movement of the jaw, i.e. ability to protrude the lower teeth in front of the upper teeth;
- thyromental distance (chin to thyroid notch): this should be >6 />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


