26
Orthopaedic anaesthesia
Orthopaedic anaesthesia encompasses a range of operations, from minor procedures on young patients (e.g. arthroscopy) to the commonly performed joint replacements (hip and knee, often in elderly patients) and major spinal surgery, including those with unstable fractures. Urgent orthopaedics cases include open fractures and neurovascular deficit.
The anaesthetist must pay particular attention to the following during orthopaedic operations:
- Great care must be taken to ensure that the patient’s airway is secure and that the endotracheal tube (ETT) or LMA being used is securely fastened so as to prevent dislodgement, especially when access to the head and neck during the operation might be difficult, e.g. under surgical drapes or when prone.
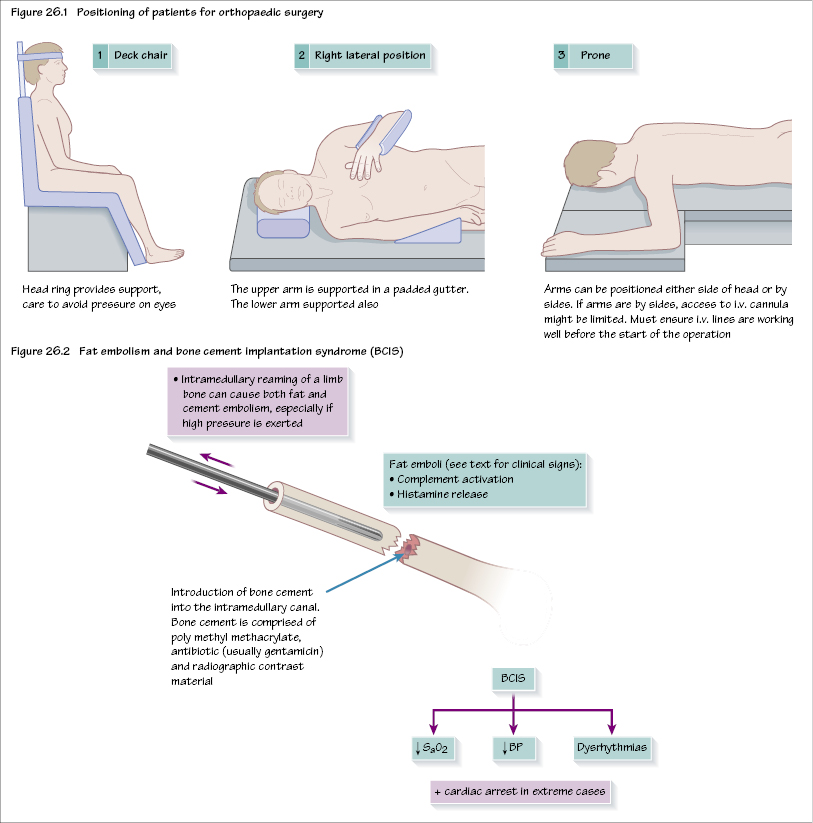
- Pressure points must be protected to prevent nerve or soft tissue damage. The use of gel pads, as well as padding and supports, helps avoid this.
- Direct pressure on the orbit must be avoided at all times in order to avoid retinal artery thrombosis and visual impairment postoperatively.
- The patient’s limbs must not be over stretched (e.g. shoulder) so as to avoid nerve plexus injury (e.g. brachial plexus palsy).
- Do not abduct the upper arm >90 degrees from body as this might cause posterior shoulder displacement.
Preoperative care
Assessment
Early fracture fixation relieves pain and is a reason for taking patients to theatre as soon as is appropriate. Patients need to be fully assessed and often require optimizing before their operation, especially the elderly, with specific attention to:
- fluid resuscitation
- anaemia
- electrolyte imbalances
- normothermia.
Medical conditions
Some musculoskeletal conditions present more commonly for orthopaedic procedures (e.g. rheumatoid arthritis (RA), osteoarthritis and ankylosing spondylitis).
Problems can include:
- Pain: even positioning an awake patient in the anaesthetic room might exacerbate joint symptoms. Pain can markedly limit exercise tolerance.
- Airway and cervical spine: up to 80% of RA patients have neck involvement, including instability and subluxation. Care must be taken when moving the head and neck position as well as transferring patients.
- Temporomandibular joint involvement can reduce mouth opening, hindering intubation or laryngeal mask insertion.
- Extra-articular disease might be present, e.g. restrictive lung disease and cardiac involvement (rare).
- Current medication must be reviewed, e.g. if taking corticosteroids, extra steroid might need to be given in the perioperative period.
The cause of a fall must be established to differentiate between a simple trip, an alcohol or drug-related fall, and those due to cardiovascular or cerebrovascular causes (e.g. postural hypotension, transient ischaemic attack or dysrhythmia)/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


