Speech, language and swallowing
Sarah Starr

Introduction
The ability to communicate effectively is vital to a person’s functioning in society. Speech and language acquisition is a developmental process occurring most dramatically in the first years of life but one that proceeds throughout a person’s lifetime. Difficulties may be encountered at any point during the language acquisition process. Children may experience problems acquiring the sounds of the language, learning how to combine words meaningfully or comprehending others’ questions and instructions. In all cases, a speech and language pathologist is the primary healthcare professional responsible for the identification and treatment of individuals with communication problems. Paediatric dentists should be aware of the symptoms and problems associated with communication impairment, particularly when it relates to orofacial or dentofacial anomalies. They should know how to refer children and their families to a speech pathologist.
Communication begins at birth and continues throughout a child’s life through adolescence and into adult life. A child’s communication development is influenced by many variables, including neurological status and motor development, oromotor status (anatomical and physiological), cognition, hearing, birth order, environment, communication modelling and experiences, as well as their personality.
This chapter will briefly describe some of the main communication disorders that can present with particular focus for paediatric dentists.
Communication disorders
There are six main areas to be considered when assessing a child’s communication:
Oral motor and feeding problems
Problems in this area constitute the earliest at which children are referred to a speech pathologist. Significant problems can result when an infant does not develop control of the oral mechanism sufficient for successful feeding. Early reflex development typically facilitates feeding behaviour, but neuromotor factors, prematurity, cleft lip and palate, long-term non-oral feeding and other reasons may interfere with a child’s development of the movement patterns essential for sucking, swallowing and feeding. Since these patterns form the scaffolding of movement for early speech sound development, children with a history of feeding difficulties may have subsequent difficulties in producing sounds for speech.
Reasons for referral
• Sucking, swallowing or chewing difficulties.
• Gagging, coughing or choking with feeds.
• Moist vocal quality during or after feeds.
• Persistent drooling (not coincident with teething).
• Presence of a craniofacial malformation.
• Parental report of feeding difficulty or refusal.
• Poor oral intake and associated poor weight gain in infants and young children.
Articulation
Articulation refers to the production of speech sounds by modification of the breath stream using the various valves along the vocal tract: lips, tongue, teeth and palate. Problems in these areas can vary from a fairly mild distortion of sounds such as a lisp, where the child’s speech is still easy to understand, through to a more severe speech production problem where all speech attempts are unintelligible or where the child makes very few speech attempts. Errors can be classified in the following ways:
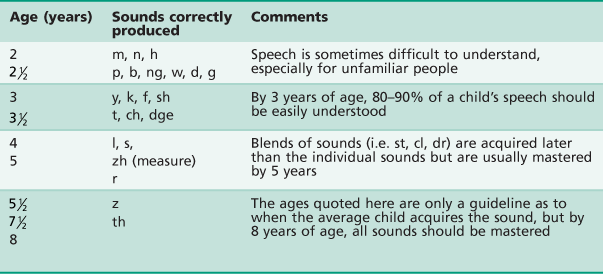
Children learn to produce sounds in a developmental sequence, with adult-like sound systems expected by 8 years of age (Table 16.1). For example, it is quite acceptable for a 2-year-old to mispronounce an ‘s’ sound, but it would be considered a problem if a similar error were made by a 7-year-old child.
Language
In contrast to the fairly straightforward examples listed above to illustrate speech sound learning, language development is much more complex. Skills emerge in two parallel levels.
Receptive language
This is the ability to understand language.
Expressive language
This refers to the ability to produce verbal and non-verbal communication in the form of words and sentences and may include speech and written language.
A child with a language disorder may present with difficulties in both comprehension and expression of language or in only one area of language learning. Language learning proceeds in a predictable order but there is more variability in the emergence of these skills than the acquisition of speech sounds. Vocabulary grows as does a child’s ability to progressively understand more complex language. Words are combined into phrases and eventually sentences, and comprehension becomes more adult-like over time. Eventually, language that is heard and said becomes the language of literacy, reading and writing. School success is highly correlated with language learning, especially in the early years.
Children may experience language learning problems at any stage of the acquisition process. There may be:
• Difficulties interpreting the meaning of words and gestures.
• Delays in the production of first words and phrases.
• A lack of understanding of questions and instructions.
• An inability to produce sentences that are grammatically correct.
A delay at any single stage may not necessarily constitute a longstanding problem, although it should be investigated further. Problems with language acquisition are the most subtle indicators of difficulties with childhood development and therefore, should never be ignored.
Voice
Voice is produced when the vocal cords in the larynx are vibrated. Changes in air flow and the shape of the vocal folds can affect loudness, pitch and voice quality. Once voice is produced, its tone (resonance) and quality is modified by the throat, oral and nasal cavities. A child with a voice problem may present with the following:
Abnormal voice quality
Rough, breathy or hoarse voice in the absence of upper respiratory tract infection.
Abnormal resonance
Hypernasality (excessive nasal tone usually due to problems closing the velopharyngeal port during speech) or hyponasality (lack of nasal resonance usually due to some type of nasopharyngeal obstruction).
Inappropriate loudness levels
Voice too soft to be heard or so loud that it is distracting from the message of the speaker.
Problems with pitch
Pitch too high or low for age or sex.
Voice problems may be caused by:
• Poor vocal use, e.g. excessive yelling or screaming (in some cases producing vocal nodules).
• Neurological problems (e.g. cerebral palsy).
• Vocal pathology such as polyps or cysts.
• Vocal irritants such as exposure to smoking, chemicals or aerosol sprays.
• Physical conditions including cleft palate, laryngectomy and hearing loss.
Fluency
Fluency refers to the smooth flow of speech. Where there are interruptions in the flow of speech, stuttering occurs. Many children experience brief periods of stuttering as they learn to speak in longer sentences and this early form of disfluency is not considered a disordered pattern, as it will usually pass. Early developmental disfluency is best resolved by reacting to the message the child is attempting to convey rather than the disfluency. When stuttering persists beyond the n/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


