16 Rubber Dam
The legacy of the dentist Sanford C. Barnum was founded on March 15, 1864, when he punched a hole in a sheet of rubber and stretched it over a mandibular molar. That day represented the beginning of the dental rubber dam—a term long used in the construction and shipbuilding industry for the isolation of a cavity from moisture. Decades later, with the development of improved suction techniques, the rubber dam became less important in the field of dentistry. However, the isolation of a tooth with a rubber dam to achieve a totally dry field of work remains an absolute clinical requirement for endodontic treatment. The European Society of Endodontics (ESE) guidelines (2006) give the following reasons for use of the rubber dam:
• prevention of salivary and bacterial contamination;
• elimination of the risk of aspiration and swallowing of instruments;
• prevention of spillage of irrigating solutions into the oral cavity.
There are a few exceptions to these basic requirements, but they seldom occur in daily practice.
Unfortunately, even today there is debate about the purpose and clinical rationale behind the preparation of a dry field using a rubber dam. The arguments against using a rubber dam are many: It takes too long to apply; patients do not readily accept it; patients become nervous and are irritated by it; it is no longer a “contemporary” dental device; endodontic treatment can be performed quite well without the rubber dam; etc. However, all the reasons for not using the rubber dam are not able to withstand critical evaluation. Studies such as those by Stewardson and McHugh (2002) clearly demonstrate that the vast majority of patients readily accept the use of a rubber dam, independent of age, gender, type of dental treatment, time of application, length of the appointment, or position of the dam.
In 1908, the veritable “grandfather” of dentistry, Dr. G. V. Black, wrote in his book Operative Dentistry: “probably no other technique, instrument or treatment in dentistry had been more universally accepted and advocated, and yet is so universally ignored by practicing dentists. Many reasons can be given but in most cases the fundamental cause is inadequate explanation and training in the dental schools. If any operative technique is not clearly taught and seen to be efficiently executed by the teachers, the new members of the dental profession will not use it willingly.”
European universities have accepted this tenet, and reports indicate, for example, that 91.6% of all German dental schools routinely use rubber dam for dental treatment (Baumgartner, 2003). However, 15 years ago, only 5% of surveyed dentists in Germany used the rubber dam, and 65% never used it (Winkler, 1991). In a 1997 study by Maier, 17.5% of German dentists regularly used the rubber dam. Most recent studies in Germany indicate that 8.2% of dental practitioners routinely use rubber dam, and an additional 25.3% use it in more than half of cases (Baumgartner, 2003).
From an international perspective, the USA is at the top: 59% of general dentists and 92% of endodontists reported that they always use rubber dam (Whitten et al., 1996). In contrast, 31% of Swiss dentists reported regular use of rubber dam, but 69% never used it (Barbakow et al., 1995). In Great Britain, 60% of dentists never used the rubber dam (Whitworth et al., 2000), and in Belgium 64.5% never used it (Hommez et al., 2003).
It has long been acknowledged that root canal treatment must be carried out under sterile conditions, because bacteria are always the cause of endodontic disease or its progression (Kakehashi et al., 1965; Sjögren et al., 1997). Keeping in mind these scientific facts and clinical practicalities, the rubber dam remains a simple, quickly applicable, and effective tool in endodontics.
The Rubber Dam
A 15 × 15 cm (6 × 6 in) sheet of rubber is the most frequently used rubber dam for clinical use. The raw material—as with latex gloves—is the sap of the native rubber tree. Chemically, the substance is a cis-1.4 polyisoprene. The material is available in five different thicknesses; in endodontics the medium, strong, and extra strong sheets are most commonly used.
Because latex allergies are quite commonly encountered, and have been observed during endodontic procedures (Chin et al., 2004), various manufacturers do provide either artificial latex (Isodam Non-latex) or latex-free rubber dam material (Flexidam Non-latex).
During endodontic treatment procedures, usually only a single tooth at a time is isolated, and so just one hole, positioned slightly off-center in the rubber dam sheet, is often all that is required. If additional teeth or groups of teeth need to be isolated, templates are available for orientation of the holes. The Ivory rubber dam punch is the instrument of choice for making appropriate holes in the rubber dam for clinical application. Although the use of special lubricants, Vaseline, or even shaving soap has been proposed, patient comfort is most easily ensured by using lip balm or placing a soft cloth barrier between the rubber dam sheet and the face/lips.
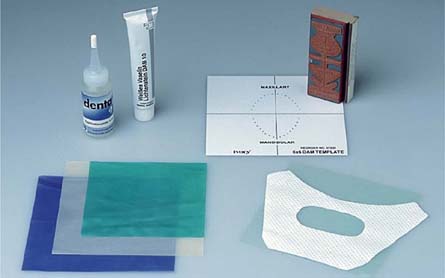
16.1 Basic rubber dam armamentarium
Latex rubber is available in various thicknesses and colors. The size is usually approx. 13 x13 cm (5 × 5 in) (green) or approx. 15 x 15 cm (6 × 6 in) (blue, cream). The cloth napkin prevents direct contact between the rubber sheet and the skin. Most recently, silicone rubber dam sheets (light green, Roeko) have become available for patients with latex allergy.
Use of lubricating agents (Dentaglide, Sigma Dental) or Vaseline makes application of the rubber dam easier. Templates simplify positioning of the hole punch in the sheet.

16.2 Rubber dam punches
The Ainsworth punch (left), with a hinge located behind the punch plate, has remained unchanged for almost 100 years, and offers the ability to make perforations in five different sizes.
The Ivory punch (right) is the best instrument for punching the rubber dam. Because of its design it is possible to punch a hole much further toward the center of the rubber dam sheet. The hinge is positioned in front of the punch plate, which permits almost perpendicular and therefore exact punching.

16.3 Punching
Left: Close-up view of the Ivory rubber dam punch showing the movable punch plate with six hole sizes ranging from 1mm to 2 mm.
Right: Making a single hole off center in one of the four quadrants (approximately 4–5 cm from the edge) simplifies placement of the rubber dam in all four quadrants: The material is turned to the left or to the right to use the hole for a maxillary or mandibular tooth. This also permits the assistant to dispense with a template and punch the holes identically for all regions.
Rubber Dam Clamps
In the earliest configurations of the rubber dam, the sheet was held in place with wooden wedges or dental floss. Soon a myriad of clamps became available designed for use on individual teeth or groups of teeth. Today, stainless-steel clamps are the most commonly used, but plastic is also available.
The rubber dam clamp needs to engage the tooth at certain critical contact points. The clamp is meant primarily for retention of the rubber dam, which it does through its spring action below the height of contour of a tooth. It may also help to slightly retract the gingiva. Currently, the following rubber clamp types are universally recognized:
• normal clamp (with wings);
• wingless clamp;
• distal clamp;
• anterior tooth, premolar, and molar clamps;
• cervical or labial clamps;
• retention clamps (for retention of the rubber dam sheet);
• retraction clamps (for gingival retraction, e.g., Brinker tissue retractor, Schultz clamps).
An exception is clamp size 212, which provides both retention and retraction.
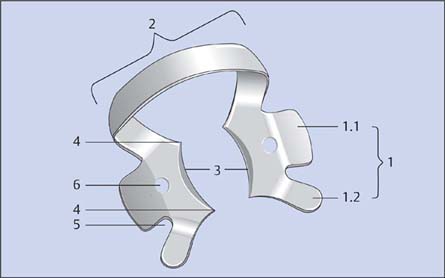
16.4 Parts of a rubber dam clamp
1 Clamp wings (lingual and buccal) with:
1.1 Central arm
1.2 Anterior arm
2 Clamp bow (distal)
3 Clamp beaks
4 Contact points
5 Notch
6 Clamp holes
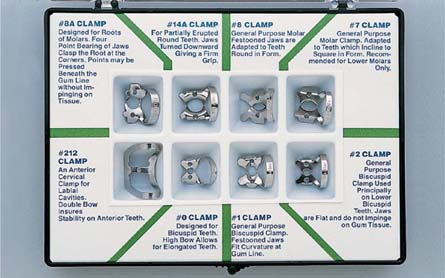
16.5 Clamp selection
As there are numerous manufacturers providing many different types of rubber dam clamp, the selection process is not always easy. Clamp sets can help in orientation. The selection portrayed here, from Ivory, consists of eight types:
8A Molar (also for broken down crowns)
14A Molar, partially erupted
8 Maxillary molars
7 Mandibular molars
212 Anterior teeth
0 Premolars (high bow)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


