Complex Amalgam Restorations
Review of Pertinent Material Qualities and Properties
The properties, advantages, and limitations of amalgam are discussed in Chapter 13 and Online Chapter 18. Amalgam is easy to use and has a high compressive strength, excellent wear resistance, and proven long-term clinical performance. It has a metallic color, does not strengthen the tooth, and does not bond to tooth structure and therefore requires a retentive tooth preparation.
Indications
Complex posterior amalgam restorations should be considered when large amounts of tooth structure are missing and when one or more cusps need capping (Fig. 16-1).1 Complex amalgams can be used as (1) definitive final restorations, (2) foundations, (3) control restorations in teeth that have a questionable pulpal or periodontal prognosis, or (4) control restorations in teeth with acute or severe caries. When determining the appropriateness of a complex amalgam restoration, the factors discussed in the following sections must be considered.

Resistance and Retention Forms
In a tooth with severe caries or existing restorative material, any undermined enamel or weak tooth structure subject to fracture must be removed and restored. Usually, a weakened tooth is best restored with a properly designed indirect (usually cast) restoration that prevents tooth fracture caused by mastication forces (see Chapter 17). In selected cases, amalgam preparations that improve the resistance form of a tooth can be designed (Fig. 16-2).
Status and Prognosis of the Tooth
A tooth with severe caries that might require endodontic therapy or crown lengthening or that has an uncertain periodontal prognosis often is treated initially with a control restoration. A control restoration helps (1) protect the pulp from the oral cavity (i.e., fluids, thermal stresses, pH changes, bacteria), (2) provide an anatomic contour against which gingival tissue may be healthier, (3) facilitate control of caries and plaque, and (4) provide some resistance against tooth fracture (or propagation of an existing fracture). (See Chapter 2 for caries-control rationale and techniques.)
Role of the Tooth in Overall Treatment Plan
The restorative treatment choice for a tooth is influenced by its role in the overall treatment plan. Although complex amalgam restorations are used occasionally as an alternative to indirect restorations, they often are used as foundations for full coverage restorations. Abutment teeth for fixed prostheses may use a complex restoration as a foundation (Fig. 16-3). Extensive caries or previous restorations on abutment teeth for removable prostheses generally indicate an indirect restoration for the resistance and retention forms and for development of external surface contours for retention of the prosthesis. A tooth may be treated with a complex direct restoration if adequate resistance and retention forms can be provided. For patients with periodontal and orthodontic problems, the complex restoration may be the restoration of choice until the final phase of treatment, when indirect restorations may be preferred.

Occlusion, Esthetics, and Economics
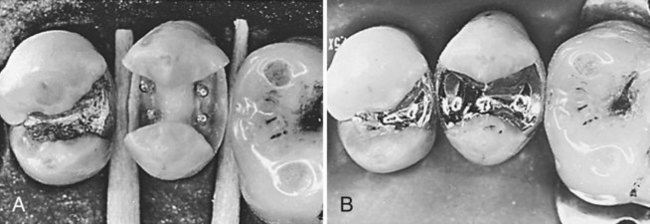
Complex amalgam restorations are sometimes indicated as interim restorations for teeth that require elaborate occlusal alterations, ranging from vertical dimension changes to correcting occlusal plane discrepancies. When esthetics is a primary consideration, a complex amalgam restoration may not be the treatment of choice because of the display of metal. When cost of indirect restorations is a major factor for the patient, the complex direct amalgam restoration may be an appropriate treatment option, provided that adequate resistance and retention forms are included (Fig. 16-4).

Clinical Technique
Initial Procedures: Summary
Pin-Retained Amalgam Restorations
A pin-retained restoration is defined as any restoration requiring the placement of one or more pins in dentin to provide adequate resistance and retention forms. Pins are used whenever adequate resistance and retention forms cannot be established with slots, locks, or undercuts only.5 The pin-retained amalgam is an important adjunct in the restoration of teeth with extensive caries or fractures.6 Amalgam restorations including pins have significantly greater retention compared with restorations using boxes only or restorations relying solely on bonding systems.7 However, caution is indicated when using pins. Preparing pinholes and placing pins may create craze lines or fractures and internal stresses in dentin.8–10 Such craze lines and internal stress may have little or no clinical significance, but they can be important when minimal dentin is present. Pin retention increases the risk of penetrating into the pulp or perforating the external tooth surface. The use of pins decreases the tensile and horizontal strength of pin-retained amalgam restorations.11,12
Slot-Retained Amalgam Restorations
For a complex restoration, a slot is a horizontal retention groove in dentin (Fig. 16-5). Slot retention can be used in conjunction with pin retention or as an alternative to it.13
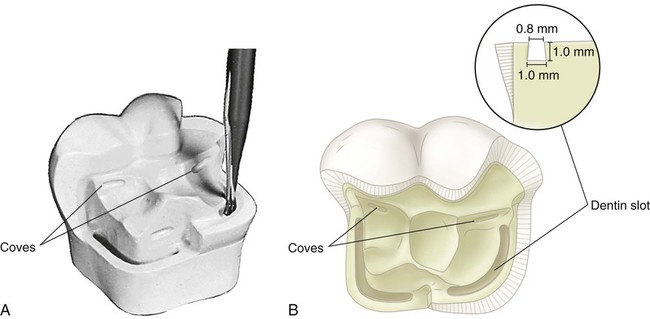
Figure 16-6 illustrates the use of coves (placed with a No.  bur) to provide additional retention form in a preparation that uses pins. Coves also may be used in preparations using slots (see Fig. 16-5). Proximal locks, as described in Chapter 14, also are placed in the proximal box and in other locations where sufficient vertical tooth preparation permits (Figs. 16-7 and 16-8).
bur) to provide additional retention form in a preparation that uses pins. Coves also may be used in preparations using slots (see Fig. 16-5). Proximal locks, as described in Chapter 14, also are placed in the proximal box and in other locations where sufficient vertical tooth preparation permits (Figs. 16-7 and 16-8).

 bur, where appropriate.
bur, where appropriate.

 round or No. 169L bur, where appropriate.
round or No. 169L bur, where appropriate.Some operators use slot retention and pin retention interchangeably. Others more frequently use slot retention in preparations with vertical walls that allow retention locks to oppose one another. Pin retention is used more frequently in preparations with few or no vertical walls. Slots are particularly indicated in short clinical crowns and in cusps that have been reduced 2 to 3 mm for amalgam.13 Compared with pin placement, more tooth structure is removed in slot preparation. Slots are less likely to create microfractures in dentin, however, and to perforate the tooth or penetrate into the pulp. Medium-sized self-threading pins may elicit an inflammatory response if placed within 0.5 mm of the pulp, whereas slot placement does not.14 The retention potential of pins and slots is similar.15–18
Amalgam Foundations
As a rule, foundations are placed in anticipation of a full-coverage indirect restoration. Not all teeth with foundations, however, need to be immediately restored with full-coverage crowns. For example, amalgam can be used as a definitive partial-coverage restoration if only minimal coronal damage has occurred in endodontically treated teeth.19 The greatest influence on fracture resistance is the amount of remaining tooth structure.20
Tooth Preparation
Tooth Preparation for Pin-Retained Amalgam Restorations
Initial Tooth Preparation
The general concept of the initial tooth preparation is presented in Chapter 14, and it applies to the pin-retained complex amalgam restorations described here. When caries is extensive, reduction of one or more of the cusps for capping may be indicated. For cusps prone to fracture, capping of cusps reduces the risk of cusp fracture and extends the life of the restoration.21,22 Complex amalgam restorations with one or more capped cusps have documented longevity of 72% after 15 years and show no differences in the survival rate of cusp-covered and non–cusp-covered amalgam restorations, whether or not pins were used.4,23
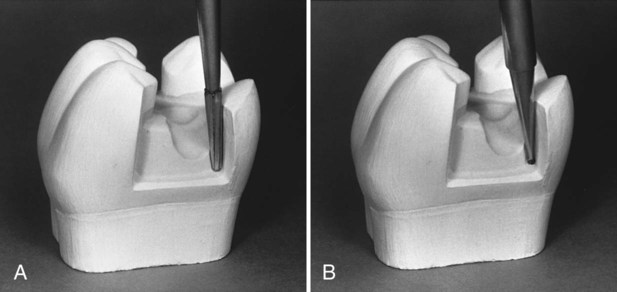
When the facial or lingual extension exceeds two-thirds the distance from a primary groove toward the cusp tip (or when the faciolingual extension of the occlusal preparation exceeds two-thirds the distance between the facial and lingual cusp tips), reduction of the cusp for amalgam usually is required for the development of adequate resistance form (Fig. 16-9, A). Reduction should be accomplished during the initial tooth preparation because it improves access and visibility for subsequent steps. If the cusp to be capped is located at the correct occlusal height before preparation, depth cuts should be made on the remaining occlusal surface of each cusp to be capped, using the side of a carbide fissure bur or a suitable diamond instrument (see Fig. 16-9, B). The depth cuts should be a minimum of 2 mm for functional cusps and 1.5 mm for nonfunctional cusps.24 To correct an occlusal relationship, if the unreduced cusp height is located at less than the correct occlusal height, the depth cuts may be less. Likewise, if the unreduced cusp height is located at more than the correct occlusal height, the depth cuts may be deeper. The goal is to ensure that the final restoration has restored cusps with a minimal thickness of 2 mm of amalgam for functional cusps and 1.5 mm of amalgam for nonfunctional cusps (see Fig. 16-9, C), while developing an appropriate occlusal relationship.
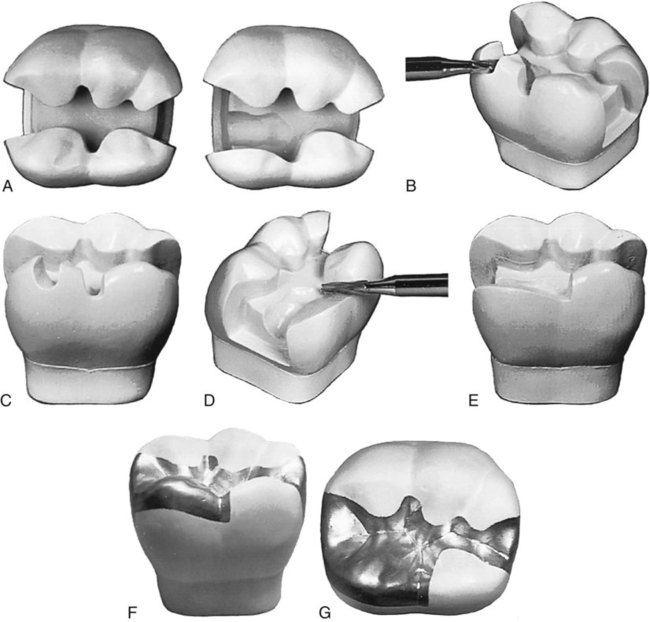
Using the depth cuts as a guide, the reduction is completed to provide for a uniform reduction of tooth structure (see Fig. 16-9, D). The occlusal contour of the reduced cusp should be similar to the normal contour of the unreduced cusp. Any sharp internal corners of the tooth preparation formed at the junction of prepared surfaces should be rounded to reduce stress concentration in the amalgam and improve its resistance to fracture from occlusal forces (see Fig. 16-9, E). When reducing only one of two facial or lingual cusps, the cusp reduction should be extended just past the facial or lingual groove, creating a vertical wall against the adjacent unreduced cusp. Figure 16-9, F and G, illustrates a final restoration. The procedure for capping the distolingual cusp of a maxillary first molar is illustrated in Figure 14-68. Extending the facial or lingual wall of a proximal box to include the entire cusp is indicated only when necessary to include carious or unsupported tooth structure or existing restorative material. The typical extension of the proximal box for restoring an entire cusp is illustrated in Figures 14-69 and 14-70, B.
Final Tooth Preparation
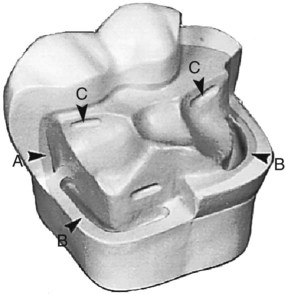
Pins placed into prepared pinholes (also referred to as pin channels) provide auxiliary resistance and retention forms. Coves and retention locks should be prepared when possible (Figs. 16-10, and 16-11). Coves are prepared in a horizontal plane, and locks are prepared in a vertical plane. These locks and coves should be prepared before preparing the pinholes and inserting the pins. Cusp reduction significantly diminishes the retention form by decreasing the height of the vertical walls. When additional retention is indicated, pins may be inserted in carefully positioned pinholes, thus increasing retention. Slots may be prepared along the gingival floor, axial to the dentinoenamel junction (DEJ) instead of, or in addition to, pinholes (see Fig. 16-10, B). Slot preparation is discussed later in this chapter.
 bur.
bur.Types of Pins
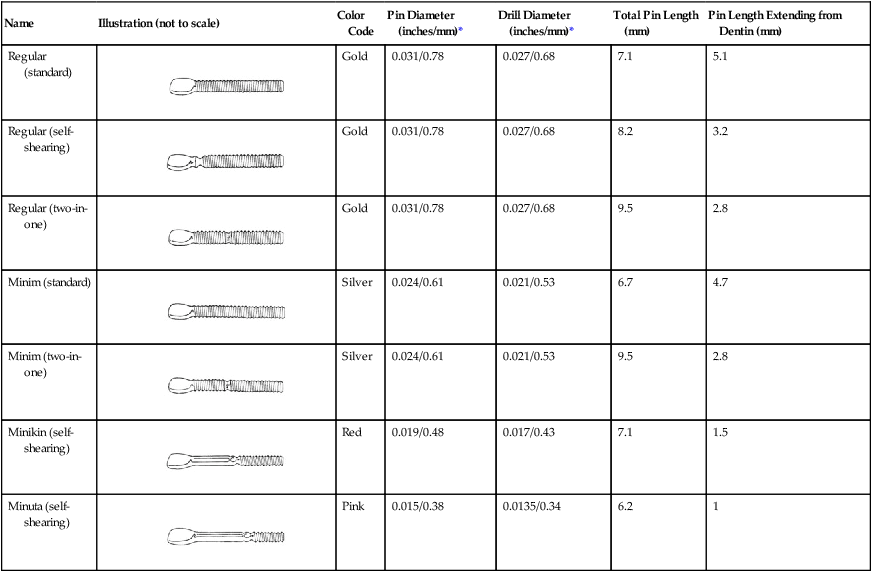
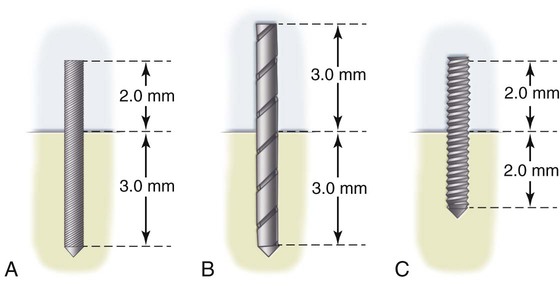
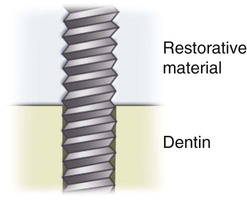
The most frequently used pin type is the self-threading pin. Friction-locked and cemented pins, although still available, are rarely used (Fig. 16-12). The pin-retained amalgam restoration using self-threading pins originally was described by Going in 1966.25 The diameter of the prepared pinhole is 0.0015 to 0.004 inch smaller than the diameter of the pin (Table 16-1). The threads engage dentin as the pin is inserted, thus retaining it. The elasticity (resiliency) of dentin permits insertion of a threaded pin into a hole of smaller diameter.26 Although the threads of self-threading pins do not engage dentin for their entire width, self-threading pins are the most retentive of the three types of pins (Fig. 16-13), being three to six times more retentive than cemented pins.27–29
Table 16-1
The Thread Mate System (TMS) Pins
| Name | Illustration (not to scale) | Color Code | Pin Diameter (inches/mm)* | Drill Diameter (inches/mm)* | Total Pin Length (mm) | Pin Length Extending from Dentin (mm) |
| Regular (standard) |
 |
Gold | 0.031/0.78 | 0.027/0.68 | 7.1 | 5.1 |
| Regular (self-shearing) |
 |
Gold | 0.031/0.78 | 0.027/0.68 | 8.2 | 3.2 |
| Regular (two-in-one) |
 |
Gold | 0.031/0.78 | 0.027/0.68 | 9.5 | 2.8 |
| Minim (standard) |
 |
Silver | 0.024/0.61 | 0.021/0.53 | 6.7 | 4.7 |
| Minim (two-in-one) |
 |
Silver | 0.024/0.61 | 0.021/0.53 | 9.5 | 2.8 |
| Minikin (self-shearing) |
 |
Red | 0.019/0.48 | 0.017/0.43 | 7.1 | 1.5 |
| Minuta (self-shearing) |
 |
Pink | 0.015/0.38 | 0.0135/0.34 | 6.2 | 1 |
Vertical and horizontal stresses can be generated in dentin when a self-threading pin is inserted. Craze lines in dentin may be related to the size of the pin. The insertion of 0.031-inch self-threading pins produces more dentinal craze lines than does the insertion of 0.021-inch self-threading pins.30 Some evidence suggests, however, that self-threading pins may not cause dentinal crazing.26 Pulpal stress is maximal when the self-threading pin is inserted perpendicular to the pulp.31 The depth of the pinhole varies from 1.3 to 2 mm, depending on the diameter of the pin used.32 A general guideline for pinhole depth is 2 mm.
Several styles of self-threading pins are available. The Thread Mate System (TMS) (Coltène/Whaledent Inc., Mahwah, NJ) is the most widely used self-threading pin because of its (1) versatility, (2) wide range of pin sizes, (3) color-coding system, and (4) greater retentiveness.33,34 TMS pins are available in gold-plated stainless steel or in titanium. Other titanium alloy pins (Max system, Coltène/Whaledent Inc.) are available.
Factors Affecting Retention of the Pin in Dentin and Amalgam
Orientation, Number, and Diameter
In general, increasing the number of pins increases their retention in dentin and amalgam. The benefits of increasing the number of pins must be compared with the potential problems. As the number of pins increases, (1) the crazing of dentin and the potential for fracture increase, (2) the amount of available dentin between the pins decreases, and (3) the strength of the amalgam restoration decreases.35,36 Also, as the diameter of the pin increases, retention in dentin and amalgam generally increases. As the number, depth, and diameter of pins increase, the danger of perforating into the pulp or the external tooth surface increases. Numerous long pins also can severely compromise condensation of amalgam and amalgam’s adaptation to the pins. A pin technique that permits optimal retention with minimal danger to the remaining tooth structure should be used.37
Pin Placement Factors and Techniques
Pin Size
Four sizes of TMS pins are available (Fig. 16-14), each with a corresponding color-coded drill (see Table 16-1). Familiarity with drill sizes and their corresponding colors is necessary to ensure that a proper-sized pinhole is prepared for the desired pin. It is difficult to specify a particular size of pin that is always appropriate for a particular tooth. Two determining factors for selecting the appropriate-sized pin are the amount of dentin available to receive the pin safely and the amount of retention desired. In the TMS system, the pins of choice for severely involved posterior teeth are the Minikin (0.019 inch [0.48 mm]) and, occasionally, the Minim (0.024 inch [0.61 mm]). The Minikin pins usually are selected to reduce the risk of dentin crazing, pulpal penetration, and potential perforation. The Minim pins usually are used as a backup in case the pinhole for the Minikin is over-prepared or the pin threads strip dentin during placement and the Minikin pin lacks retention. Larger-diameter pins have the greatest retention.38 The Minuta (0.015 inch [0.38 mm]) pin is approximately half as retentive as the Minim and one-third as retentive as the Minim pin.33,34 It is usually too small to provide adequate retention in posterior teeth. The Regular (0.031 inch [0.78 mm]), or largest-diameter, pin is rarely used because a significant amount of stress and crazing, or cracking, in the
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


