CHAPTER 16 Case Presentations
Quad Zygoma
Preliminary Presentation
The implants are placed in a “stacked” manner, with the superior implant emerging at the cuspid position and the inferior implant emerging in the bicuspid position (Figures 16-1 and 16-2).
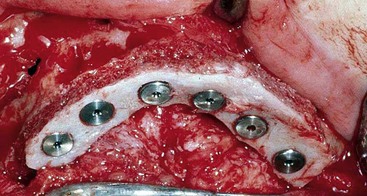

FIGURE 16-2 Placement of two zygoma implants within the body of the zygoma in a “stacked” configuration.
The preoperative panoramic radiograph demonstrates a lack of maxillary alveolar bone in all three zones. The surgical protocol for implant placement is very similar to the single zygoma implant protocol, with the exception that care must be taken to identify the most inferior lateral corner of the infraorbital rim. This reference is used while preparing the superior osteotomy to avoid penetration into the bony orbit. The implants are stabilized at 40 Ncm or greater. The two-stage protocol is followed by securing cover screws and submerging the implants for the 6-month osseointegration period (Figures 16-3 to 16-6).
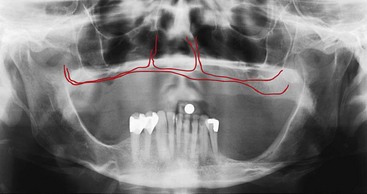
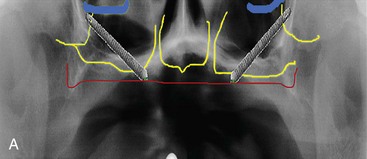
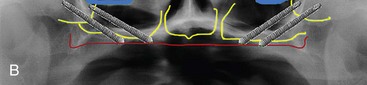
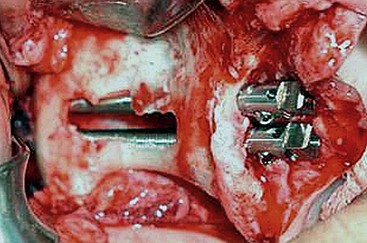
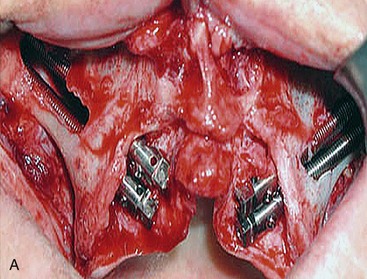

FIGURE 16-6 A, Completed surgical procedure. B, Postoperative radiograph with cover screws in place.
The completed fixed provisional is secured to the multiunit abutments and the patient’s occlusion is checked for bilateral group function. Radiographs taken after stage II surgery confirm complete seating of all components (Figures 16-7 to 16-9).
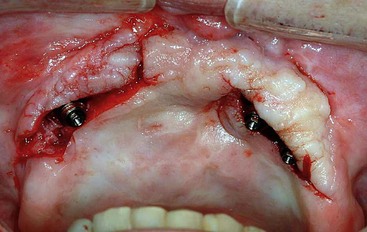
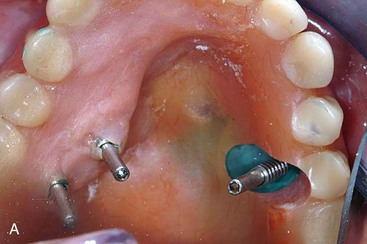


FIGURE 16-8 Placement of multiunit abutments and conversion of the full denture into a provisional fixed prosthesis.

The soft tissues are allowed to heal for a period of 6 to 8 weeks prior to initiation of the fabrication steps for the final profile prosthesis (Figures 16-10 to 16-12).





Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


