The quality of radiographic images and quality assurance
Introduction
The factors that can affect the quality of radiographic images depends on:
The effects of poor radiographic technique are the same whatever type of image receptor is used. These technique errors have already been covered in detail in relation to the three main projections used in dentistry, namely: periapicals (Ch. 7), bitewings (Ch. 8) and panoramic radiographs (Ch. 12).
The creation of the visual digital image was described in Chapter 3, together with how computer software can be used to alter and manipulate the image with regards to contrast, brightness (degree of blackening), magnification, inversion, enhancement and pseudocolourization.
Creation of the black/white/grey image on film using chemical processing was also described in Chapter 3. These various images can, however, be affected by many other factors. This chapter therefore is designed for revision, bringing together and summarizing from earlier chapters all these various factors. It also includes a quick reference section as an aid to fault-finding of film-captured images. Various image faults are illustrated together with their possible causes. This is followed by a section on quality assurance and suggested quality control measures.
Film-based image quality
As mentioned in Chapter 1, image quality and the amount of detail shown on a radiograph depend on several factors including:
Contrast
Image geometry
As mentioned and illustrated in Chapter 1, the geometric accuracy of an image depends upon the position of the X-ray beam, object and image receptor (film or digital) satisfying certain basic geometrical requirements:
Characteristics of the X-ray beam
The ideal X-ray beam used for imaging should be:
• Sufficiently penetrating to pass through the patient, to a varying degree, and react with the film emulsion to produce good contrast between the various black, white and grey shadows (see earlier)
• Parallel, i.e. non-diverging, to prevent magnification of the image (see Ch. 3)
• Produced from a point source to reduce blurring of the image margins and the penumbra effect (see Ch. 3).
Image sharpness and resolution
• Geometric unsharpness including the penumbra effect (see above)
• Motion unsharpness, caused by the patient moving during the exposure
• Absorption unsharpness – caused by variation in object shape, e.g. cervical burn-out at the neck of a tooth (see Chs 8 and 17)
• Screen unsharpness, caused by the diffusion and spread of the light emitted from intensifying screens (see Ch. 3)
• Poor resolution. Resolution, or resolving power of the film, is a measure of the film’s ability to differentiate between different structures and record separate images of small objects placed very close together, and is determined mainly by characteristics of the film including:
Practical factors influencing film-based image quality
Typical film faults
Examples of typical film faults are shown below and summarized later in Table 14.1.
Film too dark (Figs 14.1 and 14.2)

Film too pale (Fig. 14.3)
– Faulty X-ray equipment, e.g. timer
– Incorrect exposure time setting by the operator
– Failure to keep timer switch depressed throughout the exposure
– Inadequate time in the developer solution
– Developer solution too dilute
Film with inadequate or low contrast
Image unsharp and blurred (Fig. 14.4)

• Movement of the patient during the exposure (see also Chs 7, 8 and 12)
• Excessive bending of the film packet during the exposure (see also Ch. 7)
• Poor film/screen contact within a cassette
• Film type – image definition is poorer with indirect-action film than with direct-action film
• Speed of intensifying screens – fast screens result in loss of detail
• Overexposure – causing burn-out of the edges of a thin object
Film marked (Fig. 14.5)
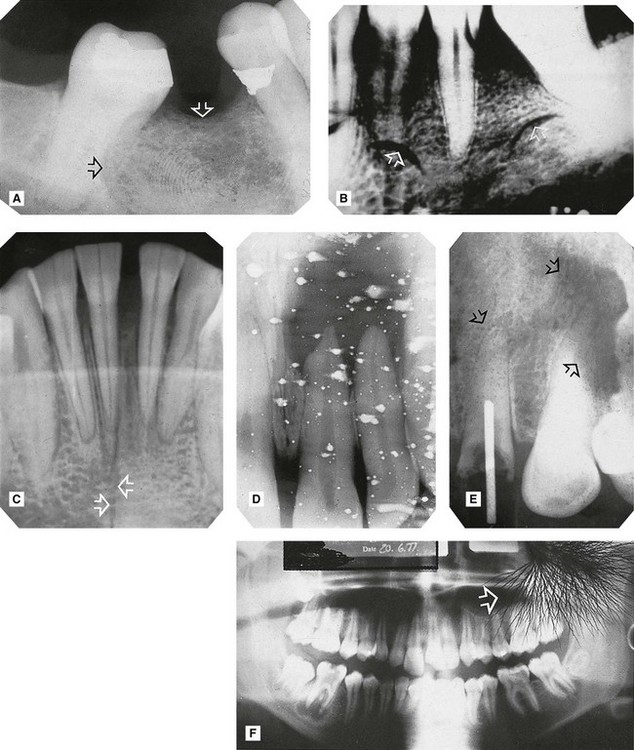
Fig. 14.5 Examples of marked films.
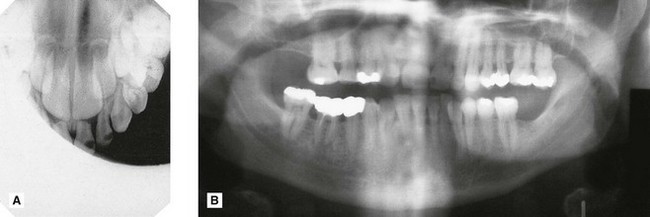
Patient preparation and positioning (radiographic technique) errors (Fig. 14.6)
These errors can happen whatever image receptor is being used and were described in detail and illustrated in Chapters 7, 8 and 12. They are summarized below and can be divided into intraoral and panoramic technique errors.
Intraoral technique errors
• Failure to position the image receptor correctly to capture the area of interest
• Failure to position the image receptor correctly causing it to bend (if flexible) creating geometrical distortion
• Failure to orientate the image receptor correctly and using it back to front
• Failure to align the X-ray tubehead correctly in the horizontal plane causing:
• Failure to align the X-ray tubehead correctly in the vertical plane causing:
• Failure to instruct the patient to remain still during the exposure with subsequent movement resulting in blurring
• Failure to set correct exposure settings (image too dark or too pale – see earlier)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


