Chapter 14
Soft Tissue Management Around Dental Implants
INTRODUCTION
Implant therapy has evolved significantly during the last two decades, from being one of the treatments of choice for edentulous arches to becoming a routine procedure to replace lost dental elements, regardless of the type of edentulism (Adell et al. 1981). With this development, the objective of implant therapy has expanded from the functional restoration of the missing dentition to include the re-creation of the lost hard and soft tissues (Garber & Belser 1995).
Only when a close resemblance with what once existed in nature is achieved does the end result of implant therapy become a success for its ability to provide the proper masticatory function while disappearing in between the remaining natural teeth.
For an implant restoration to closely mimic the lost dental element, it is undoubtedly important to select the proper shape and color of the prosthetic tooth. Nonetheless, it is imperative to surround the crown with healthy, gingival-like tissue (Figs. 14.1–14.4).
Figure 14.1. Preoperative buccal view.The first premolar is fractured.

Figure 14.2. Preoperative palatal view.The fracture line extends several millimeters subgingivally.

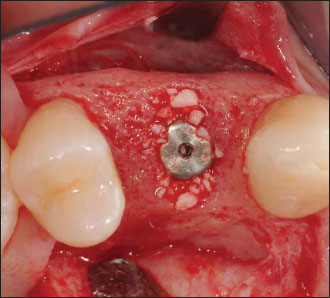
Figure 14.4. The final implant-supported restoration is in place.There is a harmonious integration of the prosthetic crown in between the natural dental elements and the healthy and natural appearance of the peri-implant gingiva.

GINGIVAL TISSUES AND PERI-IMPLANT MUCOSA
When handling the peri-implant soft tissue, it is important to acknowledge the differences that exist between the peri-implant mucosa and the gingival tissue. The mucosa that encircles the fixture has more collagen and fewer fibroblasts, with a 2:1 ratio, when compared with the periodontal gingival tissue (Berglundh et al. 1991; Abrahamsson et al. 2002).
The collagen fibers of the healthy periodontium are functionally arranged in a complex system (Smukler & Dreyer 1969), which differs from the fiber bundles of the peri-implant mucosa. The system runs mostly parallel to the titanium surface without attaching to it (Berglundh et al. 1991). It has been reported that both the titanium surface’s characteristics (Schroeder et al. 1981; Piattelli et al. 1997) and the mobility of the soft tissues (Listgarten et al. 1991) will affect the orientation of the collagen fibers. Nonetheless, even when the fibers are more perpendicularly disposed, there is no real functional insertion.
When compared with the supracrestal vessels of a natural dental element, the supracrestal vascular topography surrounding the fixture is reduced and diversely arranged (Berglundh et al. 1994; Moon et al. 1999). Both the tooth and the implant have a junctional epithelium that is approximately 2 mm long (Berglundh et al. 1991).
Despite the very similar clinical appearance between the peri-implant soft tissue and the gingiva encircling a natural dental element, the histological dissimilarities mentioned earlier bear a great responsibility in the selection of the most appropriate way to manage the peri-implant mucosa.
Encompassing the fixture is tissue, with its lower cellularity and reduced vascularity, that resembles cicatritial tissue and requires special care when surgically challenged. In the basic periodontal wound-healing processes, after flap elevation, one of the most dynamic tissues involved is the periodontal ligament (Goldman & Cohen 1980). The lack of this ligament, with its vessels and cells, must be kept in mind when approaching the peri-implant mucosa.
Although periodontal plastic procedures are used daily to correct peridental sites where mucogingival problems have already occurred, in implant therapy the less forgiving nature of the tissues involved makes it advisable initially to optimize the peri-implant soft tissues to prevent future complications.
The quality and quantity of the peri-implant tissues should be improved either before or at implant placement, during the submerged healing, or at the time of second-stage surgery (Nevins & Mellonig 1998). The outcome of some rootcoverage procedures should not be considered as predictable for implants in communication with the oral environment (one-stage implants, uncovered two-stage implants, or implants supporting a prosthesis), as they are around natural teeth (Harris 1994; Sclar 2003).
In an attempt to cover an exposed implant-abutment complex, or to mask the grayishness that transpires through thin peri-implant mucosal tissue, surgical approaches, such as the variously displaced pedicle flaps (coronally, laterally, double papilla, etc.) or free gingival autografts, usually fall short. In such unfortunate clinical scenarios, and provided that the angle of emergence of the implant-abutment-crown complex is not excessively buccal, a coronally advanced flap augmented by a subepithelial connective tissue graft represents the most predictable procedure because of its double blood supply (Langer & Langer 1985; Nelson 1987).
In particularly difficult clinical cases, removing the prosthetic components to resubmerge the fixture can be useful to widen the recipient vascular bed palatally for the subepithelial connective tissue graft. This further increases the predictability of success.
THE NEED FOR KERATINIZED TISSUE
The need for keratinized tissue around the implant is still controversial (Adell et al. 1981; Wennstrom et al. 1994; Warrer et al. 1995). Despite this, the presence of gingival-like tissue has several important advantages. The keratinized gingival tissue provides a tight fibrous collar that surrounds the implant, sealing off the bacteria from the depth of the peri-implant sulcus (Warrer et al. 1995).
The several restorative maneuvers that precede the crown placement are potentially detrimental to tissue health, and the presence of immobile keratinized tissue seems, at least from an immediate clinical perspective, to better withstand the trauma that is caused. Also this allows for easier plaque control for the patient and during periodic maintenance recall visits (Figs. 14.5–14.9).
Peri-implant tissue that resembles the keratinized gingiva on the adjacent natural teeth is important in the aesthetic zone. The free autogenous gingival graft (Sullivan & Atkins 1968) still represents the preferred procedure to predictably increase the keratinized soft tissue that encircles the implant.
The tissue that forms around the transmucosal portion of the implant, though initially considered similar to the dentogingival junction (Berglundh et al. 1991), often limits the predictability of achieving ideal soft tissue profiles. This is particularly true in the interimplant areas, where the presence or absence of the papillae determines the final aesthetic result (Tarnow et al. 2003).
Figure 14.5. Preoperative view.The patient, treated with an implant-supported restoration 12 years ago, now complains about discomfort during daily oral hygiene procedures.

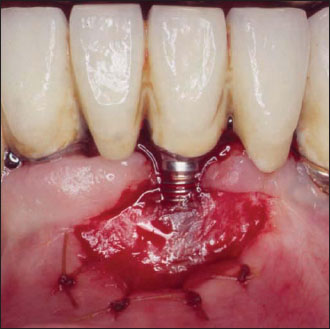
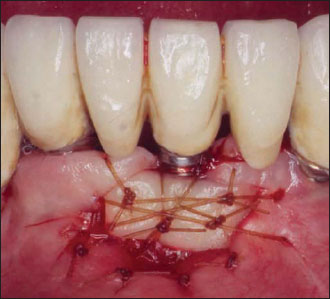
Figure 14.8. Final healing of the area.The patient did not experience any further discomfort during brushing. An unexpected creeping attachment phenomenon of about 2 mm was also obtained.

BIOLOGICAL WIDTH AND GINGIVAL BIOTYPES
This traditionally refers to the sum of two histological peridental entities: the junctional epithelium and the connective tissue attachment (Gargiulo et al. 1961; Vacek et al. 1994). The importance of these two distinct, but related, tissues within the environment of the dentogingival junction has been amply debated in the literature (Maynard & Wilson 1979; Smukler & Chaibi 1997).
The integrity of the dental biological width (average histological value, 2.04 mm) protects, by its biological sealing property, the other underlying deep periodontal tissues that are kept separated from the outer oral and sulcular environment (average histological value, 0.69 mm) (Listgarten et al. 1991).
Figure 14.9. After 3 years, during a periodical hygiene recall, stability of the area is evident. The creeping phenomenon progressed for an additional 0.5 mm (compare with Fig. 14.8).

Known for its high histological variability, the biological width together with the gingival sulcus coincide to form the different clinical periodontal biotypes (Weisgold et al. 1997), more recently redefined as periodontal phenotypes (Muller & Eger 2002). The main, and most immediate, clinical expression of the periodontal biotype is related to the degree of scalloping of the gingival tissues. The outline of the gingiva and its scalloping reflect the osseous morphotype of the underlying supporting osseous crest (Vacek et al. 1994).
The dental anatomy, with its convexities and concavities, also affects both the soft and the hard tissues that peak in the tooth surface depressions and fall in areas of surface protuberance (Olsson et al. 1993; Becker et al. 1997; Smukler & Chaibi 1997).
Whereas the gingiva and the osseous crest normally run parallel to each other, and to the tooth cemento-enamel junction buccally and lingually (or palatally) in the interproximal area, the position of the gingival tissues is affected by other variables and may or may not follow the osseous crest profile (Smukler & Chaibi 1997). Factors such as the position of the adjacent dental elements and their anatomy that determine the shape and location of the contact point, together with the interproximal peak of bone, influence papillary form and height (Tarnow et al. 1992).
Under normal circumstances, the height of the soft tissue column, located interproximally, is superior to the height of the soft tissue column located buccally (Kois 1996). This further magnifies the degree of gingival festooning that tends to flatten out toward the posterior sextants of the mouth. Some authors have speculated on the variation in the extent of the biological width and sulcus depth in the different periodontal biotypes (Muller & Eger 2002).
Despite the academic interest in these observations, it is relevant to remember that, irrespective of the degree of scalloping (periodontal biotype), the biological width of a tooth is invariably located supracrestally. The fibers of the connective tissue attachment, functionally inserted into the cementum as Sharpey’s fibers, support the gingival margin and the papilla (Fig. 14.10). In other terms, the papilla, supported by the interproximal peaks of bone, can climb higher as a result of the additional support from the connective tissue attachment to the tooth.
Knowledge of the peculiar histological and anatomical features of the dentogingival junction, which differ from those of the peri-implant mucosa, is fundamental to match the patient’s expectations. A clinician must anticipate, before beginning therapy, the potential cosmetic limitations in certain known clinical scenarios.
AESTHETIC PREDICTABILITY
The re-creation of ideal soft tissue profiles (particularly in the papillary areas) around implants is more predictable in areas of single edentulism then in multiple implant sites (Salama et al. 1998; Grunder 2000; Garber et al. 2001; Tarnow et al. 2003) (Figs. 14.11–14.13).
Figure 14.10. The sum of the connective tissue attachment (CTF) and the junctional epithelium (JE) forms the biological width (between the black arrows). A biological width around a tooth forms above the crest of bone differently from what we have surrounding an implant where it forms below the level of the bone.
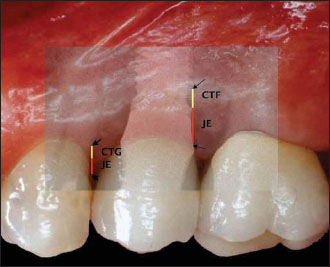
Figure 14.11. Preoperative view. A single implant is planned to replace the missing central incisor. A severe horizontal osseous deficiency was noted at computed tomography, and a chin-graft procedure was selected for the osseous reconstruction prior to implant placement.

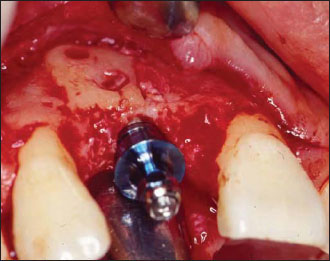
Figure 14.13. Final restoration in place. The patient did not wish to recreate the original diastema with which he was born, and preferred a slight mesiodistal discrepancy between the two centrals. Note the almost ideal gingival scalloping.

Smukler et al. (2003a & b), discussing single implants in the aesthetic zone, stress the difference between the length of interproximal soft tissue on the implant side (4–6.5 mm/ implant platform-top of the papilla) and the same distance on the adjacent tooth side (3–4.5 mm/interproximal osseous peak-top of the papilla). It is now widely accepted that, under such clinical circumstances, the interproximal osseous crest on the adjacent natural tooth maintains the height of the papilla (Salama et al. 1998; Grunder 2000; Smukler et al. 2003a & b).
The presence of a thick and flat biotype increases the predictability of a pleasant aesthetic result. Thick tissues are more resistant to the controlled traumatic injuries caused during dental treatments, and a lower degree of scalloping in the gingiva is more easily replicable at the end of implant therapy. For similar reasons, it is easier to replace a missing tooth in a periodontally treated patient (flat biotype) and obtain soft tissue profiles that are in harmony with the remaining natural dentition (Figs. 14.14–14.16). The possibility of predictably re-creating an ideal gingival outline between two or more contiguous implants has been questioned (Tarnow et al. 2003) (Figs. 14.17–14.22).
Whenever the rehabilitation involves two or more lost teeth, the osseous profile of the edentulous area, matched by the gingival profile, is no longer scalloped but either flat or, even worse, concave. As a result, the precious interproximal osseous septum that normally supports the papilla is no longer available. It is now possible, and advisable, to transform a concave edentulous ridge into a flat one by guided bone regeneration (Simion et al. 1994; Jovanovic & Nevins 1995).
In the best-case scenario, we will start from a flat osseous anatomy into which the implants will be inserted. A proper mesiodistal spacing of the fixtures (at least 3 mm) will grant the maintenance of the interimplant bone height (Salama et al. 1998). This interimplant peak of bone is often more apically located than the one that was present before the loss of the natural dental elements. Additionally, the two contiguous implants do not have Sharpey’s fibers functionally inserted into the cementum to support the supracrestal soft tissue (Tarnow et al. 2003).
The biological width around two-stage implants ad modum Branemark always forms subcrestally (Berglundh & Lindhe 1996). In this process, bone is resorbed (360° around the neck of the implant) and replaced by connective tissue fibers. Whether this is the result of the biological width forming (Berglundh & Lindhe 1996) or due to the cupping phenomenon caused by the bacterial contamination of the microgap (Hermann et al. 1997, 2000), the final result does not change. The connective tissue encircles the fixtures subcrestally differently than it does around natural teeth, where the supracrestal connective tissue fibers further support the verticality of the gingival tissue (Tarnow et al. 2003).
Figure 14.14. Preoperative view. The right central incisor is fractured and scheduled for extraction and immediate implant placement.The crown of the right lateral incisor is fractured as well, and a composite resin restoration will be done. Note the flat and thick biotype and the marginal recession of the gingival tissues.

Figure 14.15. Immediate implant placement at the time of extraction.

Figure 14.16. Final restoration in place. Despite a slight marginal disharmony between the two centrals, the overall aesthetic result is acceptable because of the generalized gingival recession pattern and the flat biotype of the patient.

Figure 14.17. Preoperative view of the maxillary and mandibular left sextants.The maxillary first premolar and second molar are hopeless. The second mandibular molar should also be extracted. Multiple implants are planned for both the maxilla and the mandible.

When considering that the average height, according to the most recent available data (Tarnow et al. 2003), of the interimplant tissue, measured from the interimplant peak of bone to the tip of the papilla, is 3.4 mm, it is easy to understand the aesthetic limitations encountered when placing two adjacent implants in the cosmetic zone.
ONE-PIECE IMPLANTS VERSUS TWO-PIECE IMPLANTS
Recent investigations of one-piece nonsubmerged implants (ITI implants; Straumann, Basel, Switzerland) have shown different patterns in the way bone heals around the fixture when compared with two piece implants (Hermann et al. 2001). According to the authors, the presence of a microgap in a two-piece implant in the vicinity of the osseous crest would determine an increased resorption of bone when compared with a one-stage one-piece implant (Figs. 14.23–14.26).
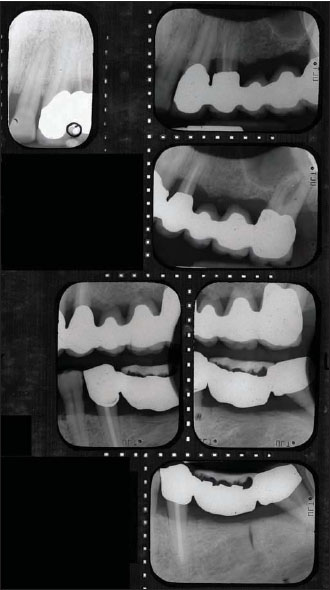
Figure 14.18. Radiographs of the area reveal the extent of the periodontal pathology and the ill-fitting restorations.

In the 1990s, investigations conducted on animals in Sweden demonstrated how multiple disconnections and reconnections of the implant abutment were followed by a more apical relocation of the peri-implant connective tissue band (Abrahamsson et al. 1997). The average biological width measured for a one-piece implant (2.84 mm) would be similar to the width around a natural tooth (2.7 mm + 3 mm = biological width + sulcus depth) and generally smaller than the width measured around a two-piece implant (Ericsson et al. 1996; Hermann et al. 2001). The Brånemark-type of implant would additionally be characterized by a more apical location of the gingival margin when compared with an ITI type of fixture (Hermann et al. 2001).
Despite the evidence presented by the research, which was conducted on a dog model, we must not forget that one-piece, one-stage implants were also included in the investigation conducted by Tarnow et al. (2003) on 136 interimplant papillae measuring an average of 3.4 mm.
Figure 14.21. Final implant-supported restorations in place.The function of the area was successfully regained with patient satisfaction.Two PFM (porcelain fused to metal) crowns were replaced on the maxillary canine and the mandibular second premolar.There is flatter gingival scalloping and the absence of papillae that are commonly found around multiple adjacent implants.

Figure 14.22. Postoperative radiograph. The interimplant peaks of bone were preserved after the 360° peri-implant osseous resorption took place. Despite that, no “real” papillae are clinically present (see Fig. 14.21).The nice radiographic result obtained after simultaneous sinus elevation on the last maxillary implant is clearly visible (compare with Fig. 14.18).
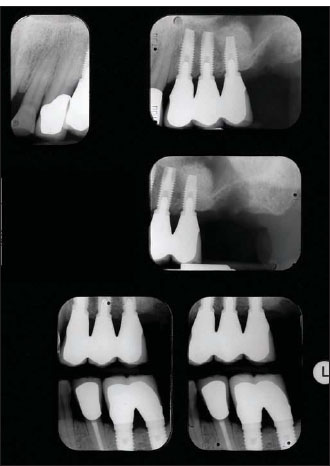
Figure 14.23. Radiograph showing the typical peri-implant osseous resorption pattern around two-piece implants. Usually bone resorbs 360° around the implant platform for a depth of approximately 2 mm.
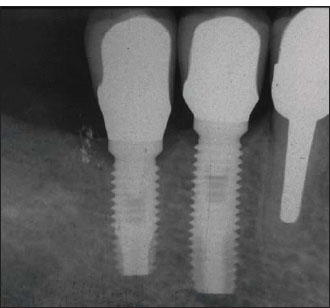
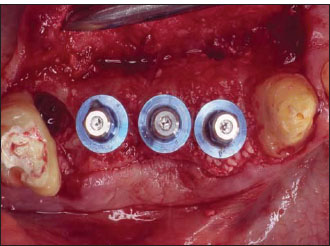
Figure 14.24. Clinical view of the two implants shown in Fig. 14.23.

According to the value reported by Kois (1996), the average papillary height in natural dentition is usually around 4.5 mm, about 1 mm more than measurements between implants. Furthermore, the interimplant peak of bone, despite advancements obtained with osseous regenerative procedures, is commonly found to be more apical than the original interdental osseous crest. This is particularly true in the presence of a scalloped periodontal biotype.
To improve the aesthetic result in the cosmetic zone, the ITI type of fixtures are commonly sunk more apically to obtain transmucosal space that is used to develop an ideal anatomical profile with the prosthetic components that connect to the otherwise unanatomical round platform of the implant. In doing so, the rough-smooth interface of the implant is buried deeper into the bone and, according to the research by Hermann et al. (1997, 2000), this determines a larger circumferential loss of crestal bone. Under these circumstances, the differences, if any, between one-stage or two-stage implants are minimal.
Figure 14.25. Radiograph showing the peri-implant osseous resorption pattern around a one-piece transmucosal implant (compare with Fig. 14.23). Although the resorption pattern is certainly different from that of a two-stage type of implant, a narrower cupping defect is still apparent.
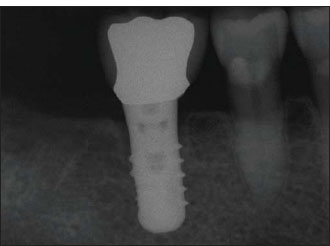
Figure 14.26. Clinical view of the implant shown in Fig. 14.25.

In the attempt to overcome the limitations, new scalloped fixture designs have been proposed (Holt et al. 2002) and recently introduced into the market (Wöhrle 2003). More research is still needed to validate the benefits claimed with the use of the designs.
With the knowledge that crestal bone remodels away, both vertically and horizontally, from the implant-abutment interface (Tarnow et al. 2000), several clinicians have successfully managed to minimize the peri-implant osseous cupping by moving the microgap inward. This clinical intuition has been recently defined as the platform switching technique and can be easily accomplished (with certain implant types) by downsizing the diameter of the abutment (e.g., 4-mm abutment platform) in relation to the supporting implant diameter (e.g., 5-mm implant platform) (Figs. 14.27–14.29).
In the author’s own experience, this still anecdotal, easily performed, clinical trick has been proven to reduce the extent of the peri-implant crestal bone loss significantly, at least from a radiological standpoint (Figs. 14.30 & 14.31).
It is relevant to note how some implant manufacturers have, in the past, designed their fixtures with a coronal bevel that brings the abutment to sit inside the implant platform. Research comparing this latter design (Astra Tech implants; Astra Tech, Waltham, MA, USA) with the more traditional Branemark fixture produced controversial results regarding differences in the amount of crestal bone resorption (Puchades-Roman et al. 2000; Hermann et al. 2001; Astrand et al. 2004).
Independent from the significance of the compared average values of the vertical osseous loss around the two systems, there was common agreement on the different initial pattern of bone remodeling noted for the beveled platform (Puchades-Roman et al. 2000; Hermann et al. 2001). This observation may lead more implant companies to shape their two-stage implants in such a way that could even out the discrepancy, in terms of biological width dimensions, with the one-piece transmucosal fixtures (Hermann et al. 2001). It has yet to be determined to what extent this might affect the peri-implant soft tissue profiles and the aesthetic predictability of implants.
Figure 14.27. According to the platform-switching technique, a 4-mm-diameter abutment is used on a 5-mm-diameter implant platform. In the picture, an anatomical custom abutment has been manufactured.

Figure 14.28. Clinical view of the implant shown in Fig. 14.27.

Figure 14.29. Radiograph of the implant depicted in Fig. 14.27. Note how the platform-switching approach seems to abate the amount of peri-implant bone loss.
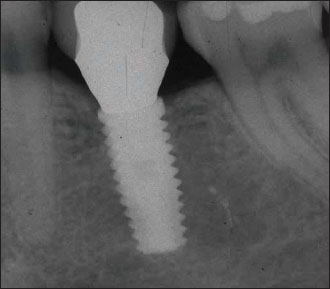
Figure 14.30. Radiograph showing two maxillary implants realized according to the platform-switching concept. No apparent cupping defects are visible.

Figure 14.31. Clinical view of the maxillary implants shown in Fig. 14.30.

UNCOVERING TECHNIQUES
When a submerged approach is selected, a second surgery is performed for several purposes: it enables the implant to be uncovered and verifies the achievement of clinical osseointegration, it enables the healing abutment or the provisional restoration to be connected to the fixture, and it represents the last chance to improve the peri-implant soft tissue. At the second-stage surgery, the site should be carefully evaluated to determine whether the quantity and quality of the soft tissues fulfill the previously planned therapy expectations.
Unfortunately, often deficits in terms of tissue volume, gingival keratinization, or both will be present. Whenever possible, adequate peri-implant keratinized tissue should be obtained by adjacent sites by using pedicle flaps (Moy et al. 1989; Hertel et al. 1994). If the surrounding anatomy does not favor the sculpting of a pedicle flap, the alternative naturally is epithelialized soft tissue grafts (Sullivan & Atkins 1968).
For buccolingual volumetric defects, modifications of the original Abrams’s roll technique can be used successfully (Abrams 1980; Scharf & Tarnow 1992; Israelson & Plemons 1993; Barone et al. 1999). The peri-implant soft tissue can also be augmented by grafting connective tissue, either before or at the time of the uncovering (Langer &/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


