14
Cleidocranial Dysplasia
Clinical features and dental characteristics
Treatment modalities
Dental crowding
Retention of the treated result
The Jerusalem approach in clinical practice
Treatment experience
Patient variation
Clinical Features and Dental Characteristics
The cleidocranial dysplasia patient is typically of short stature, with a brachycephalic skull and bossing of the parietal and frontal bones. There is hypoplasia of the mid-face, giving the misleading appearance of mandibular prognathism. The skull sutures and fontanelles exhibit delayed closure and secondary centres of ossification occur in these areas, with the formation of wormian bones. The development of the clavicles is defective and ranges from a small medial gap to total absence in severe cases [1–7]. The patient usually has a narrow chest and sloping shoulders.
According to Stewart and Prescott [8] more than 100 other anomalies have been associated with these major clinical features of the condition. Cleidocranial dysplasia does not affect the sufferer mentally or intellectually and, from this aspect, he/she is completely normal. The palate is narrow and occasionally high, and there is a marked degree of lateness in the development of the deciduous dentition, while eruption is generally normal. There is rarely any alteration in the number of the deciduous teeth, although on occasion, erupted supernumerary/supplemental deciduous teeth may be seen in the incisor area. The permanent molars usually erupt late, but spontaneously, while the remainder of the permanent dentition (i.e. the successional teeth – incisor, canines and premolars) exhibit very delayed or non-eruption. Additionally, supernumerary teeth typically develop in the successional teeth areas and much less frequently in the molar areas in numbers that may vary from none to around 12 in general. While greater numbers are uncommon in these cases, the highest recorded number reported in the literature was 63 [9]. Apart from barrel-shaped teeth and the rare occurrence of peg-shaped teeth in the maxillary incisor area only, the supernumerary teeth take the form of premolars in the premolar area, canines in the canine area and incisors in the incisor area. They may therefore be more appropriately referred to as supplemental teeth.
At the other end of the scale, the author’s experience with a large number of these cases has revealed two patients with the correct number of teeth, another with congenitally missing maxillary lateral incisors and yet another with a missing third molar.
Equally affecting males and females, cleidocranial dysplasia is an autosomal dominant inherited disease [4] and there is a high incidence of new mutations at around 20–40% of all cases [5]. Part of the RUNX family of transcription factors, RUNX2 (Runt-related transcription factor 2) is known to be the gene directly involved. It encodes a nuclear protein, 521 amino acids, (56648 Da) with a Runt DNA-binding domain. RUNX2 is essential for osteoblastic differentiation and skeletal morphogenesis, acting as a scaffold for nucleic acids and regulatory factors involved in skeletal gene expression.
RUNX2 is the only gene specific to the aetiology of CCD, with sequence analysis showing 60–70% of CCD patients present with a missense or nonsense mutations, small insertions or deletions and exon skipping. Among the remaining 30–40% of patients with mutations, 13% may be found by other means of testing (karyotype for visible deletions, insertions and rearrangements involving the RUNX2 locus in chromosome 6p21, qPCR, Real-time PCR, FISH, etc.) to have large deletions of the gene and of the genes following. Mutations in the RUNX2 gene span the whole gene and are highly penetrant.
There is no clear genotype/phenotype correlation in CCD. Although, when mutations of RUNX2 are found, they are pathognomonic of the disease and phenotypes of other diseases are not associated with them [10].
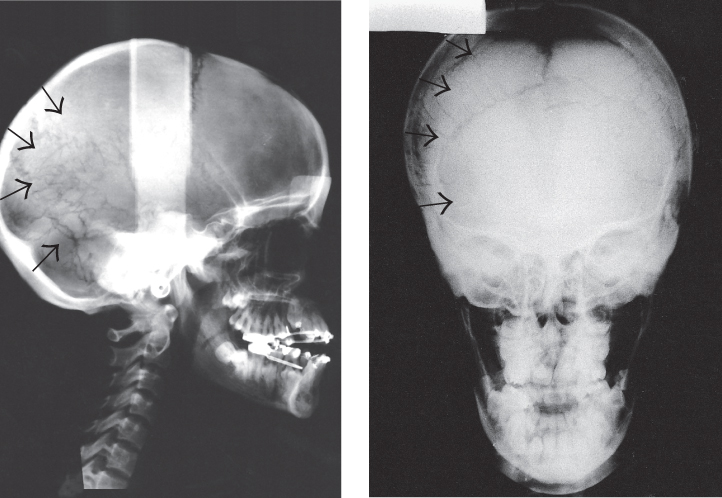
Approximately one-third of the cases we have seen have been sporadic occurrences, with no family history of the condition. Most of the cases that have been under our care come from families where a parent was affected and thus diagnosis was usually (but not always) made at birth. For most of the other cases, a tentative or initial diagnosis was suspected only several years later by the child’s paediatrician or orthopaedist, although the discovery may sometimes be made at a routine paediatric dental examination. Corroborative evidence from a clinical examination and a wider radiological examination was then obtained to establish the definitive diagnosis. During the physical examination, the clinician should attempt to confirm as many of the features described above as possible. In particular, the patient should be asked to approximate the shoulders to confirm the clavicle anomaly (Figure 14.1). Palpation should also be made of the areas between the parietal bones on the crown of the skull and between the frontal bones at the upper forehead/hairline region. In both of these midline areas, a smooth and wide hollow, concavity or furrow (Figure 14.2) may be clearly felt, in contrast to the convex contour of the skull of a normal child. Radiological examination should include views of the clavicles (Figure 14.3), the fontanelles, which may be seen on lateral and postero-anterior cephalometric films (Figures 14.4 a, b) and an initial panoramic film of the jaws (Figure 14.6).
Fig. 14.1 (a, b) The approximated shoulders of a cleidocranial dysplasia patient.
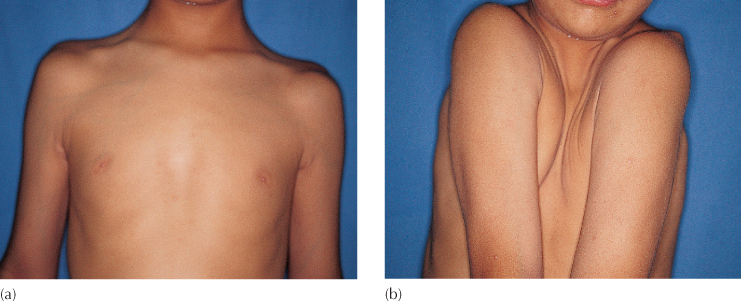
Fig. 14.2 Frontal midline furrow passing through the hairline.

Fig. 14.3 Chest radiograph to show incomplete clavicles.
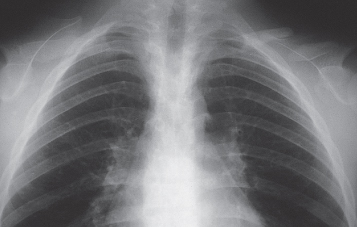
Fig. 14.4 (a, b) The postero-anterior and lateral cephalograms show abnormal cranial form, open fontanelles and numerous wormian bones (arrowed).
Aside from the principal bony defects of the cranium and clavicles, a good proportion of CCD individuals suffer other skeletal and orthopaedic anomalies. According to Cooper et al. in 2001, 57% suffer from flat feet, 28% from knock-knees and 18% from scoliosis, while joint dislocation of the shoulder and elbow may also occur [11]. Additionally, infections of the upper respiratory tract are common, specifically the sinuses and the ears, where conductive hearing loss occurs in 39% of the cases. Treatment for these associated conditions is indicated and should be performed by the paediatric specialist concerned. For the most part, the signs and symptoms of the condition are very distinct and, these predispositions aside, entirely benign. They are in no way progressive, the patient is not physically or mentally disabled and, in general, other body systems are not adversely affected.
At present, there is no way to change the underlying inherited condition, treatment cannot therefore be advised for the primary condition [5, 6] and its diagnosis does little more than label the child as an oddity. The only situation where treatment is needed is when one or more of the associated consequences become burdensome. By and large, it is the oral and dental disability of the condition that undoubtedly presents its most serious ramifications, since this affects the vertical and horizontal growth of the face and oral structures, including alveolar bone and teeth. From student to experienced practitioner in the dental profession, and out of all proportion to the rarity of the condition, its clinical features are surprisingly well known, again reflecting its curiosity value rather than any ability on the part of the profession to have been able to promote change and correction in the past. For many decades, the profession has stood in awe of the overwhelming number of the dental problems that these cases present, unable to offer satisfactory answers.
The dental characteristics typically include over-retention of the deciduous dentition, non-eruption of the permanent dentition and the presence of many supernumerary teeth (Figure 14.5). Nevertheless, there is no dental discomfort or disturbance, unless the deciduous teeth become decayed. These teeth are small relative to the growing face and are not visible below the upper lip, particularly when an often seen anterior open bite is present. In many cases, in the rest position it is the tongue that is visible between the lips (Figure 14.6). The horizontal growth pattern generally produces a mandible of normal length and an underdeveloped maxilla which therefore produces a skeletal and dental class 3 relationship. However, this relationship is not always present initially in the younger patient, but may gather momentum during the adolescent growth spurt to a greater or lesser degree [12] (Figure 14.7). This trend is by no means certain, and there are cases of good class 1 relationships and even the occasional class 2 case that may be diagnosed, as they complete the development of their facial pattern, at the end of the adolescent growth period. The vertical growth of the alveolar processes is generally deficient, which leaves the patient with very shallow labial and lingual sulci in both jaws. Taken together, these features give the patient an edentulous appearance, which may often be the presenting symptom.
Fig. 14.5 Variation in number of supernumerary teeth in cleidocranial dysplasia patients. (a) A 14-year-old female with eight extra teeth. (b) A 14-year-old female with five extra teeth. (c) A 13-year-old male with one mesiodens. (d) A 12-year-old male with a missing tooth and no supernumeraries. (e) A 14-year-old female with a full deciduous dentition and two erupted supernumerary deciduous maxillary lateral incisors. Only one erupted (deeply carious) permanent molar is present. There are 27 supernumerary teeth, in addition to the 31 unerupted permanent teeth – a total of 81 teeth! Note the presence of supplemental molar teeth.
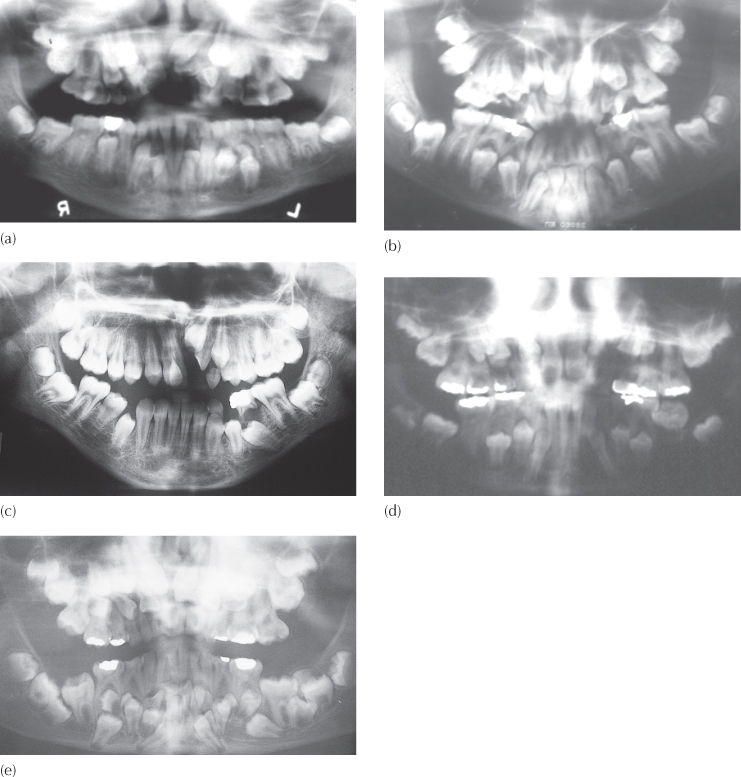
Fig. 14.6 The tongue is visible at rest, protruding between the lips.

Fig. 14.7 Typical growth in the cleidocranial dysplasia patient. (a, b) At age 10 years, the facial soft tissue profile is orthognathic, although the intra-oral dental and dental base relations are class 3. (c, d) At age 17 years, there is a clear underdevelopment of the mid-face, with an accompanying mandibular prognathism and a marked worsening of the class 3 dental and skeletal relations. The patient is being prepared for orthognathic surgery.
(Courtesy of Dr D. Harary.)
(e, f ) At age 17.5 years and following surgical correction.

Some light has been shed on a possible reason for the non-resorption and over-retention of the deciduous teeth and the non-eruption of the permanent teeth in these cases [13]. It has been proposed that decreased root surface resorption occurs in the deciduous teeth due to a thin uniform layer of resorption-resistant acellular cementum covering virtually the entire root. In the permanent teeth, very little cellular cementum is seen on the roots of the teeth. However, secondary deposition of reparative cementum is found in areas of focal resorptive defects, and this may be blamed for the non-eruption of the permanent teeth.
Given that:
1. the child with cleidocranial dysplasia has little by way of a tangible complaint involving pathology (no pain, no swelling, no difficulty in functioning), yet
2. the dentist has diagnosed a benign condition of extraordinary therapeutic magnitude,
3. the dentist has no available guidelines on how to even begin to approach the resolution of the problem,
4. a practitioner seeing a case for the first time is unable to predict treatment results, and
5. the degree of facial deformity is usually of insufficient consequence to demand surgical modification, at least in the younger patient,
it is entirely understandable that a responsible clinician will hesitate before undertaking treatment.
The options are:
- not to offer treatment at all;
- to suggest the more radical approach of extraction of many teeth, followed by prosthetic replacement; or
- to advise an orthodontic–surgical treatment procedure, with an unknown level of confidence in the ability to achieve the desired outcome.
However, non-treatment becomes less of an option as the patient grows older. Because of considerable occlusal attrition and caries there is a progressive morbidity of the deciduous dentition, which starts in the early teens and gathers pace over just a few years. Root canal treatment is often needed and restoration becomes difficult. The patient’s appearance suffers further, with a reduced lower face height [14], impaired masticatory function and continuing facial growth contributing to the increasing over-closed appearance. Treatment is needed to provide an efficient masticatory apparatus and improvements in the dental appearance and the facial proportions.
Treatment Modalities
These goals may be realized in several ways. The methods that have been proposed over a period of many years have most often reflected the particular area of dentistry in which the treating dentist has specialized. Therefore, to a degree, the mode of treatment may depend on whose door the patient first knocks!
Prosthodontics
The most popular approach has been to provide the patient with removable partial or full prostheses, which fulfil all the immediate needs of the patient. This approach has been suggested by many only after the removal of all the deciduous teeth and the unerupted supernumerary and permanent teeth [9, 15, 16]. Given that the alveolar bone height in these cases is very limited, with shallow sulci, the dentist should ponder the implications of the construction of replacement tissue-borne prostheses 10 years later, after additional and iatrogenic ridge resorption has occurred.
Others have advised retaining the standing teeth and the construction of prostheses around them [8, 16–18]. A further refinement recommends the exploitation of any standing teeth, together with the surgical exposure of the more superficial unerupted teeth, to serve as supports for an over-denture [18–20]. By making it tooth-borne, the denture is less likely to cause further ridge resorption, but the supporting teeth will deteriorate quickly under these circumstances, both from caries of their crowns and their root surfaces and from loss of their periodontal attachment.
Implant-based prosthodontics is largely ruled out because implants cannot be placed in a jaw that is full of unerupted teeth, without the removal of a very large number of these teeth. Extensive extraction will take its toll with the postsurgical resorption of additional alveolar bone from the already severely reduced bony ridge. For the most part, therefore, the relative absence of suitable implant sites and the thinness of the mandible itself will rule out the use of implants.
Surgical Relocation
In the search for a non-prosthetic method that utilizes the existing teeth, surgical removal of the supernumerary teeth, followed by careful dissection of the unerupted teeth and their repositioning or transplantation into artificially prepared sockets, has been proposed [5, 21, 22]. However, the long-term results of this method, in the context of its use in cleidocranial dysplasia, and with the presence of multiple impactions and deficient alveolar bone width, have not been investigated. This is an important area for study, since it would give the profession some inkling as to the fate of these teeth in later years. Accordingly, the practitioner seeking appropriate answers is left to ponder whether the transplanted teeth will erupt autonomously and behave like normal teeth or perhaps undergo ankylosis and root resorption in common with other transplanted teeth.
These methods all suffer one serious drawback, namely that the results thus achieved deteriorate fairly rapidly and their prognoses are relatively poor. When one considers that treatment for the condition needs to be carried out in the patient’s second decade of life, these modalities must be considered to be of limited value and essentially inadequate to the aim of lasting through to old age.
Orthodontics and Surgery
Before the mid-1960s, while some limited positive results were obtained with orthodontics, the idea was considered to be fanciful and impractical, and was widely derided. Nevertheless, it caught the imagination of a small number of clinicians, and, particularly in the late 1970s and early 1980s, several publications appeared advocating a surgical and orthodontic method. Methods were designed to bring about the eruption of the teeth by extracting the deciduous teeth, surgically removing the unerupted supernumerary teeth and exposing the buried permanent teeth, with or without the use of a surgical pack, depending on the depth of the individual teeth within the tissues [14, 23–25].
The patient was then seen in routine follow-up visits, until the teeth erupted or had reached a sufficiently accessible position, occlusal to the healed gingival tissues, for the application of orthodontic bands or bonded attachments. In other words, assisted eruption was provided only for those teeth that had already partially erupted. For CCD, characterized as it is by a lessened power of eruption, many months will pass before teeth appear and some of the more deeply sited teeth will never erupt. Additional surgical exposure is needed for some of these, but still with no guarantee of success.
Immediate bonding and ligation at the time of surgery for these cases was introduced in the literature in the 1980s, when Trimble et al. [26] and Davies et al. [27] each showed a single case in which this was done. The advantage of being able to apply forces to the most intractably impacted teeth is well illustrated in these two cases.
The results and prognosis that may be achieved by a method involving surgical removal of the unwanted deciduous and supernumerary teeth, followed by the orthodontically assisted eruption and alignment of the natural permanent teeth, must be viewed as warranting exploitation. What, after all, could be better than to restore the dentition with the patient’s own teeth and with normal alveolar bone support, through the medium of a healthy periodontal ligament?
Since the orthodontic literature records few attempts to standardize orthodontic treatment strategy beyond the above-mentioned single case reports, it must be concluded that the orthodontic option had not been exercised for many cases and that there seem to be few centres anywhere in the world where a significant number of patients had been treated. For these reasons, the present state of opinion regarding recommended or appropriate procedure is difficult to assess accurately.
Nevertheless, within this modality, three courses of action have been suggested over the years, each based on the experience of the treatment of several cases and each with its own relative merits. These will be referred to as:
- the Toronto–Melbourne approach
- the Belfast–Hamburg approach
- the Jerusalem approach.
The Toronto–Melbourne Approach
This method was originated by a team from Toronto [14] and was later further developed in Melbourne [24]. Surgical procedures are performed in a stage-by-stage series under endotracheal general anaesthesia, with the degree of root development of the permanent teeth dictating the timing of each stage. Thus, initially, the deciduous incisor teeth are extracted at 6 years of age, followed by the deciduous canines and molars at 9–10 years. Supernumerary teeth overlying the crypts of the unerupted permanent teeth are removed, together with substantial amounts of bone to uncover the crowns of the permanent teeth to their maximum diameter. The teeth are left widely exposed. The Melbourne team prefers to expose the incisors at a separate and additional surgical episode, and this is done after the first molar bands are placed following the late eruption of these teeth, which may reach full expression only at about the age of 10–11 years. Surgical packs are used to maintain the patency of the surgical exposure and to safeguard access for eventual bonding of the teeth.
The expectation is that, following the removal of the obstructive elements (i.e. the deciduous and supernumerary teeth, together with a liberal amount of bone and soft tissue), the teeth will then erupt of their own accord to a varying degree and over an extended time-frame. When convenient, orthodontic brackets are bonded to individual teeth and these are drawn to a light archwire, which spans the unsupported premolar/canine areas, from the banded molars to one or more anteriorly erupted incisors. Teeth are then drawn to the archwire, depending on their becoming accessible to bracket bonding.
Smylski et al. [14] and Hall and Hyland [24] do not propose any special or purpose-designed appliances to deal with the vertical traction that is needed in every area of the mouth, but appear to rely on conventional methods used in routine orthodontic treatment.
Limitations
In this method, the patient is under treatment for many years, starting from a very early age and requiring several recommended and fairly extensive surgical interventions, followed by several smaller ones for individual teeth. The age of the patient in the early stages and the scope of the surgery are the major determinants as to whether all these interventions should be carried out under general anaesthesia.
The deciduous anterior teeth are removed at an early stage in order to encourage the eruption of permanent incisors. Nevertheless, in their subsequent recommendation to fully expose the permanent incisor teeth in a distinct and separate surgical stage, Smylski et al. [14] and Hall and Hyland [24] recognize that spontaneous eruption does not always occur. This means that the patient is anteriorly edentulous for some considerable time. This would seem a high price to pay for what may be undue optimism regarding the potential in cleidocranial dysplasia for normal eruption. In two of the three cases described by Smylski et al. [14] unerupted supernumerary teeth were not present in the anterior segments and the permanent incisor teeth responded to simple exposure and packing. However, there are many cases where spontaneous eruption does not occur, this being one of the diagnostic criteria of the condition, which may be associated specifically with the frequent presence of supernumerary teeth in this region.
The placement of attachments to the deeply sited permanent teeth is not performed at the time of surgery, but some time later, after full healing (by secondary intention) has occurred and the surgical packs have been removed. Thus, at each surgical stage, valuable time is lost between the exposure and the force application needed to encourage the eruption of the teeth.
The Belfast–Hamburg Approach
Simultaneously, but quite independently, Richardson and Swinson [28] of Belfast and Behlfelt [29] of Hamburg proposed a diametrically opposite method of treatment of the teeth in cleidocranial dysplasia. They recognized that, while there is the need for extensive surgery in these cases, this could be completed at one time, including the extraction of all deciduous and supernumerary teeth and the exposure of all unerupted permanent teeth. This is carried out under general anaesthesia, under operating theatre conditions, and with surgical packs placed over the remaining teeth to encourage epithelialization of the exposed tissue, which is the essence of healing by secondary intention.
During the succeeding weeks, these surgical packs remain in place and are perhaps changed over a further quite short period, until brackets may be conveniently bonded to the exposed teeth. This can then be done under what the proponents consider to be more reliable conditions for bonding than those pertaining during the surgical procedure.
Whether or not eruption of these teeth occurs without assistance is the subject of some debate, with one source insisting that, while there is apparent improvement, this is due to the radical loss of surrounding soft and hard tissue during the surgical procedure rather than actual vertical dental change [30].
Nevertheless, even with the most favourable and optimistic assessment, there can be no doubt that the eruption will be neither sufficient nor reliable enough to eliminate the need for extrusive mechanics. As with the Toronto–Melbourne approach, appliances consist of molar bands and bonded brackets, with long spans of unsupported and relatively fine archwire used to vertically develop the partially erupted teeth.
Limitations
By recommending all extractions and exposures at one time, the Belfast–Hamburg surgical policy has clear advantages from the patient’s point of view, although a balance has to be struck in terms of timing. The earlier-developing permanent teeth, particularly the incisors, should not be exposed too late in their development to lose any eruptive potential that they may have, while the later-developing teeth should not be exposed too early when their roots are insufficiently developed. Accordingly, the Belfast team [28] recommends that the one-time, comprehensive, surgical intervention be performed at age 12–14 years.
The immediate advantage of this policy is very clear and encouraging, although its drawbacks are of considerable consequence and not so obvious. By delaying treatment until this late age, the teeth of the normal series will have been held deep down in basal bone by the supernumerary teeth, particularly in the lateral incisor/canine/premolar area, for an extended period of time. Their roots will have reached an advanced stage of development in these cramped circumstances, which is likely to exaggerate the tendency for a stunted, tortuous and distorted root morphology [31]. Removal of the unwanted extra teeth at this late stage will relieve the impaction of the permanent teeth of the normal series, but it will do so at a time when they exhibit even less potential for spontaneous eruption, particularly in the incisor region, since the root apices will already have been completed.
During growth in a normal child and with the eruption of permanent teeth, the vertical development of the alveolar processes that occurs makes a significant contribution to the height of the lower face. It also leads to the establishment of deep vestibular and lingual sulci, with a clear differentiation of wide zones of oral mucosa and attached gingiva. In the untreated cleidocranial dysplasia patient, vertical growth of the alveolar bone appears to be markedly diminished. This brings about the typically reduced height of the lower third of the face that is so frequently a feature of the condition.
Thus, with the late removal of the unwanted deciduous and supernumerary teeth at a time when most of the patient’s growth has already occurred, the ultimate vertical alveolar growth that accompanies the erupting permanent teeth will be correspondingly less, leaving a shallower sulcus, an absence or reduced width of attached gingiva and an incompletely vertically developed lower third of the face.
Furthermore, and in addition to removing the unwanted supernumerary teeth, it is necessary to gain access to the canine and premolar teeth of the normal series and to expose them widely. When the procedure is performed at this late stage, these target teeth are very deeply situated, often with their developing root apices close to the lower border of the mandible or the floor of the nose and maxillary sinus. This necessitates the removal of considerable quantities of bone [14] and, as recommended by several authors, the placement of a surgical pack over and around the crowns and necks of the teeth to prevent bony healing-over and to encourage spontaneous eruption. This packing procedure will markedly delay healing and is designed to prevent the reparative filling-in of bone. It is difficult under these circumstances to avoid pushing the pack into the area of the cemento-enamel junction (CEJ), which will inevitably lead to a poor periodontal prognosis for the finally erupted tooth, with an exposed CEJ and lessened bone support [32].
The frequent need to change packs over a long period incurs pain, discomfort and nuisance, difficulty in maintaining oral hygiene and a limitation of normal function, with a prolonged bad taste and odour in the mouth due to the unhygienic circumstances. From the surgeon’s point of view, this entails seeing the patient for many time-consuming appointments. There is no active encouragement of eruption until brackets may be successfully bonded and traction applied, in a case already afflicted by slow or non-eruption as a characteristic of the disease. Thus, at an age when facial appearance is very important, the patient will spend an unacceptably long time without teeth. Furthermore, bone regeneration will have been retarded by the use of a method involving healing by secondary intention [33]. Eruption is thus delayed, and a growing over of the soft tissues, to re-cover the deeper and newly exposed teeth, may still occur.
From the discussion of these two approaches, it becomes clear that treatment could be vastly improved if the placement of attachments and the initial application of extrusive traction could be included as two of the functions to be addressed during the surgical procedure. This creates several formidable obstacles, the largest of which is the ability of the surgeon to create a series of micro-environments whereby a small area of the crown of each of the teeth is exposed and conditions of haemostasis and isolation prepared, to permit the delicate attachment bonding procedure.
There can be no question that the skills needed to achieve this type of complicated treatment protocol require more than one pair of hands and more than one qualified operator in the operating theatre. The ideal situation is the interdisciplinary cooperation of the surgeon with the orthodontist at this critical time. As pointed out in Chapter 3 and in several subsequent chapters, there are enormous advantages to be gained by the presence of the orthodontist at this crucial stage, which has a long-term bearing on the efficacy of the later orthodontic resolution of impacted teeth in general. If this is true of the treatment of a single impacted tooth, then its benefit is exponentially more valuable in relation to multiple impactions, many of which are often located deep in basal bone.
Without the placement of attachments at the time of surgery, access to the unerupted teeth must be guaranteed by the surgeon performing wide opening and radical bone resection, with the placement of surgical packs. With attachment placement, a conservative surgical policy is possible – only enough bone is removed to allow access for the placement of a small eyelet attachment on the minimally exposed tooth surface. The surgery may then be aimed at preserving rather than removing bone, since the presence of bone in the eruption path does not hinder mechanically encouraged eruption of the teeth, in these cases or in general. Its lack would be a greater drawback in terms of the eventual degree of bone support and thus of the periodontal prognosis of the erupted teeth [32].
It has been reported [14] that denser alveolar bone is present in cleidocranial dysplasia. We have not found abnormal bone in any of the cases in our care, although the observer could understandably be misled by the fact that cortical bone is found, to the relative exclusion of spongiosum. It should be remembered that the impaction of many teeth within the jaws takes up much of the volume within the body of the mandible where spongiosum would normally be present. Thus, while cortical bone encompasses all these teeth and is present in normal amounts, spongiosum is sparse.
The Jerusalem Approach
This method [34, 35] was presented for the first time at the same forum as the Belfast–Hamburg approach described above [36]. Its modus operandi is quite different from either of the two other approaches. The Jerusalem approach is based on a rationale that is related to the abnormal dental development of the patient and on the factors that produce it.
This comprehensive approach to treatment addresses the following points:
- recognition of the clinical features of the facial, oral and dento-alveolar structures in the disease;
- the surgical measures that are required to provide access to the areas concerned;
- the need for an orthodontic strategy to enable the application of extrusive mechanics to the buried teeth in an efficient and reliable manner;
- attending to the patient’s psychological well-being by focusing the earliest stages of treatment on the resolution of the incisor impactions.
Recognition of the Clinical Features
Cleidocranial dysplasia patients exhibit each of the following features to a variable degree:
1. non-resorption of deciduous teeth roots;
2. the presence of supernumerary teeth, markedly displacing the developing permanent teeth and providing a physical barrier to their eruption;
3. lessened eruptive force, although eruptive movements are evident;
4. poor vertical development of alveolar bone, as witnessed by a shallow sulcus, a reduced height of the lower face and a class 3 skeletal tendency, due to an underdeveloped maxilla and to a counter-clockwise mandibular rotation;
5. late but normal and unhindered eruption of first and, much later, second permanent molars in both arches;
6. late dental development, as judged by the root development of the permanent teeth, whether erupted or unerupted – a 12-year-old patient will typically show a dental age more appropriate to that of a 9-year-old [24, 35, 37].
Surgical Therapeutic Measures
The timing regarding the actual exposure of the permanent teeth is critical, and only two interventions are planned at distinct points in time, depending on the extent of root development, as follows.
Intervention 1
At the dental age of 7–8 years, the anterior deciduous teeth, together with all the supernumerary teeth, in the anterior and, as far as reasonably p/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


