6
Palatally Impacted Canines
Prevalence
Aetiology
Complications of the untreated impacted canine
Diagnosis
Treatment timing
General principles of mechano-therapy
The need for classification of the palatal canine
A classification of palatally impacted canines
Prevalence
In any population, the prevalence of palatally impacted maxillary canines is low, but it seems to have a variable distribution with regard to ethnic origin. The lowest frequency reported in the literature relates to Japan [1], where the anomaly occurred in only 0.27% of the sample population. Some very early studies by Cramer [2] among white Americans and Mead [3] in an undefined sample found 1.4% and 1.57%, respectively. A study of a large series of full mouth dental radiographs among patients in the USA revealed a figure of 0.92% [4], while Brin et al. [5], in a study of an Israeli population, found a 1.5% prevalence. Higher figures for the anomaly have been found in more recent surveys: 1.8% was reported in the study by Thilander and Jacobson [6] of an Icelandic population, and 2.4% in an Italian sample [7].
Montelius [8] was the first to indicate a difference between Caucasian and Oriental populations, finding a frequency of 1.7% for Chinese and 5.9% for Caucasians. However, since he did not distinguish between buccal and palatal impaction in his study, little useful information may be gleaned from these figures in the immediate context. More recently, the work of Oliver et al. [9] indirectly indicated that Asians may suffer from buccally impacted canines more frequently than from palatal canines. While this appears to be supported by various case reports that have appeared in the literature from the Far East, no definitive study has been undertaken to investigate this possibility.
A strong prevalence of impacted canines is found among females, with a ratio of 2.3:1 in the above-mentioned group of American patients [4]. 2.5:1 in an Israeli orthodontic group [10] and 3:1 in each of a Welsh orthodontic group [9], a US orthodontic sample [11] and an Italian sample [7].
However, some confusion exists with regard to these figures, since a subsequent random Israeli population study [5] showed an approximately equal male–female occurrence of the anomaly. Furthermore, Oliver et al. [9] indicated that, although a higher female incidence was present in their study of Welsh patients, this reflected the trend for more females to seek orthodontic treatment in the UK.
Appearance is rarely marred by the presence of an over-retained deciduous canine, since there is a complete and uninterrupted display of teeth, and any abnormalities are usually not disfiguring. That being the case, and if we are to accept an ‘appearance/aesthetics’ motivation for girls seeking treatment more frequently than boys, then the diagnosis of an impacted maxillary canine alone does not seem to be an adequate reason for the preponderance of females seeking treatment. Motivation for treatment may therefore rather depend on the ability and persuasiveness of a particular practitioner in pointing out the potential hazards of non-treatment. There may be no basis to expect that this would convince more female patients than males to accept treatment.
Aetiology
There is no single cause for the palatal displacement of the maxillary canine tooth. Space-occupying, extraneous entities of dental origin (Figure 6.1) will undoubtedly produce abnormal positioning of an unerupted permanent maxillary canine, but they are comparatively rare in the canine area. The fact that the majority of impacted canines occur in their absence compels us to look elsewhere for the main causes of impaction. Nevertheless, when a supernumerary tooth (Figure 6.1a) or an odontome (Figure 6.1b) appears in the area, they disturb the position and orientation of a developing canine tooth and deflect the eruptive force to express itself in a futile direction. Their timely removal may sometimes bring about spontaneous re-orientation and resolution, although this is by no means certain and active orthodontic intervention is usually necessary in the final instance.
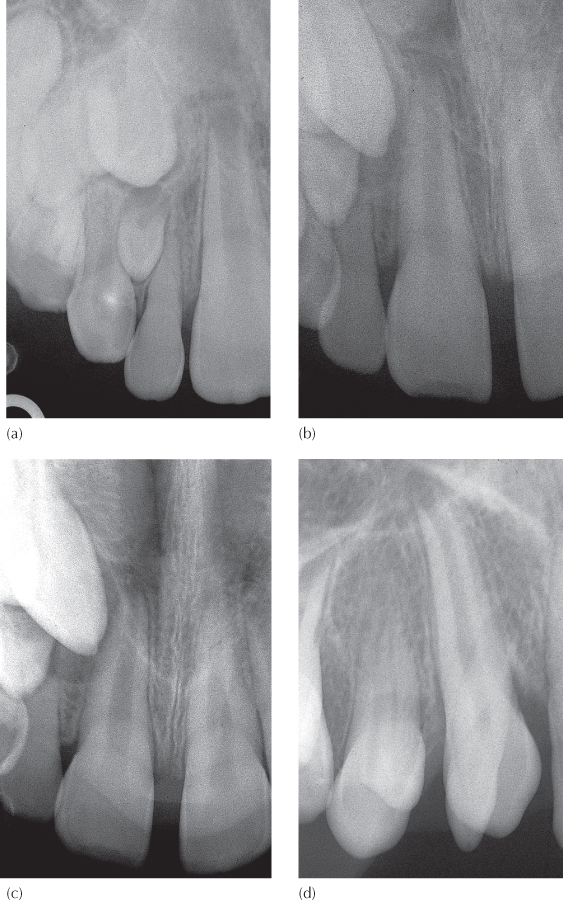
Fig. 6.1 (a) Anterior occlusal view shows an impacted canine, an odontome and a missing lateral incisor. (b) Periapical view of impacted canine and first premolar associated with an odontome and over-retained deciduous first molar. (c, d) A three-dimensional CBCT view showing the apical third of the root of a normally sited first premolar to be turned 90° to the mesial, directly in the path of the unerupted canine, which is being deflected further mesially and prevented from erupting. The transaxial (vertical) CBCT slice across the canine in the area of the CEJ and longitudinally through the deciduous canine. It also cuts across the mesio-distally oriented horizontal portion of the root close to the apex of the premolar.
(Courtesy of Dr N. Dykstein.)
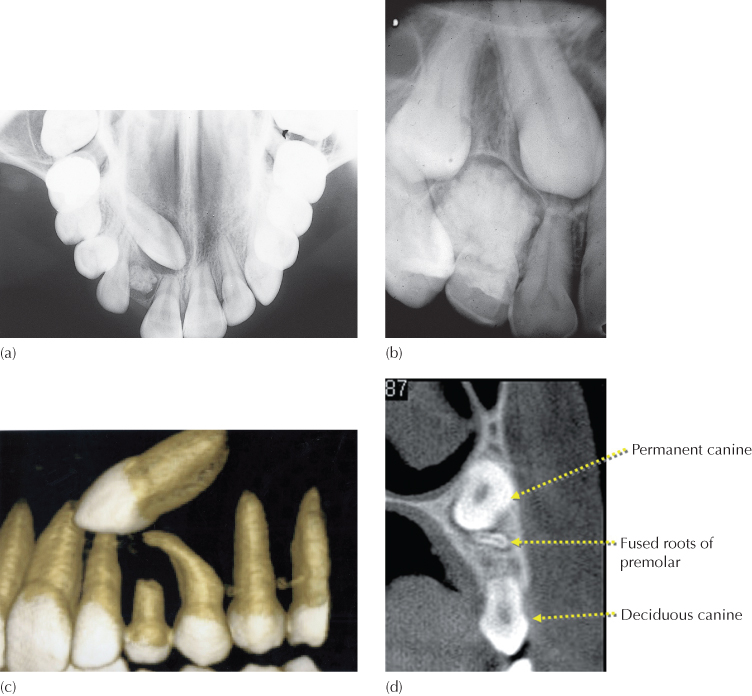
One other factor may be found in the context of premolar root morphology. An example of this is seen in Figure 6.1c, d, in which the buccal and/or palatal roots or a fused single root develops directly in the path of the unerupted canine. The canine may then become impacted, deflected or halted, but the physical presence of the canine may act as an impediment in the way of the developing root end, which may also serve to cause a mesial curving of the interfering root.
In order to resolve this impaction, the premolar root may be uprighted distally and rotated mesially, with a modicum of palatal root torque, thereby moving its root apex distally and palatally to distance it from the canine. The canine may then be exposed and mechanically erupted in the usual manner and into its ideal position. Finally, the premolar should be returned to its upright position and re-rotated as much as possible, using light force, and the effort should be discontinued immediately it meets with resistance that will be caused by contact between the mesially curved premolar root end and the canine root.
Other treatment options include:
1. Root treating and apicoectomizing the premolar and extracting the deciduous canine, which should all be done at the same time as exposure of the canine.
2. Extracting the canine and leaving the short rooted deciduous canine in place.
3. Extracting the premolar and the deciduous canine, which is an approach to be considered if the overall malocclusion may be treatment planned as a 2- or 4-unit extraction case.
To return to the more usual forms and to explain the mechanism of palatal displacement of the maxillary canine, some of the hypotheses that have been put forward have been intimately involved with aberration in the normal process by which the maxillary anterior teeth erupt. For this reason, an understanding of normal development in this area is important.
Normal Development
In the middle period of the deciduous dentition, a periapical radiograph of the premaxillary region will show the fully completed deciduous incisor roots. It will show the overlapping shadows of the permanent central and lateral incisors more or less in the same vertical plane (Figure 6.2a) and at the level of the apical area of the roots of the deciduous incisors, with the canines being sited higher up. The overlap of the permanent teeth crowns is due to the fact that these relatively wide permanent teeth are all contained in a narrow area and, at this time, are initially located palatally in the alveolus. The developmental position of the lateral incisors is palatal in relation to both the central incisors and the permanent canines. For these reasons, the periapical view described above gives the appearance of severe crowding.
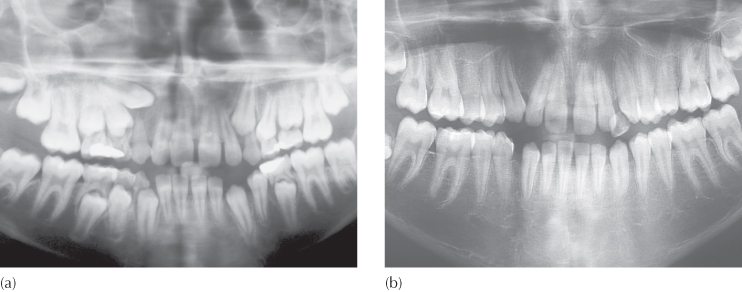
Fig. 6.2 (a) A periapical view of maxillary permanent incisors, at age 3 years. Note the degree of overlap of unerupted permanent central and lateral incisors. (b) The same patient at 5 years. The permanent central incisors have migrated inferiorly and labially relative to the lateral incisors. Note the reduced degree of incisor overlap. (c) The central incisors are erupting at age 6.5 years. Note how the lateral incisors have migrated labially into the arch to eliminate the overlap completely.
(Courtesy of Professor B Peretz.)
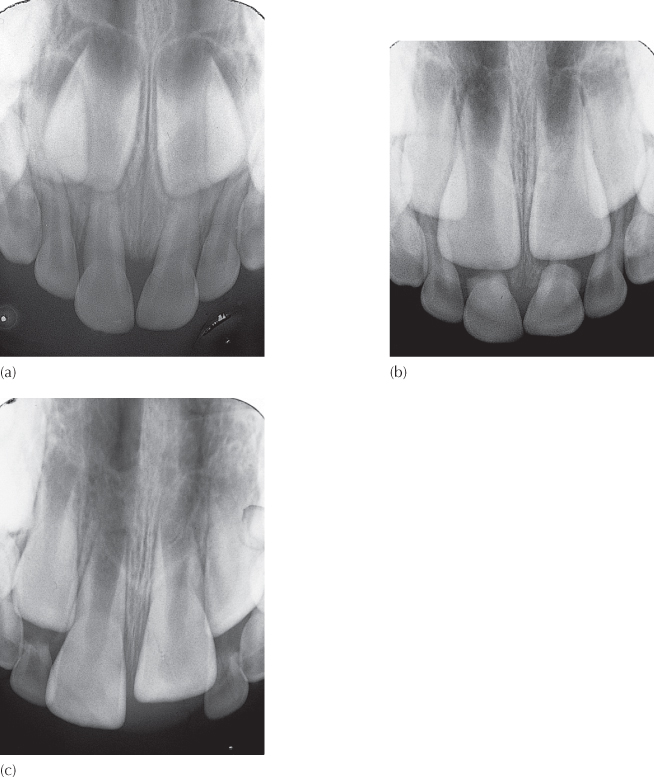
During the early eruptive movements of the central incisors, a progressive resorption of the roots of the deciduous incisors occurs. The permanent incisors migrate slowly across from the palatal side of the arch to the labial as they proceed in their downward path, until the teeth erupt into a more labial perimeter than was defined by the deciduous incisor teeth before their shedding. During this process, the wide crown portion of the central incisors will have moved downwards and labially, ahead of the lateral incisors (Figure 6.2b). As this occurs, the progressively narrower cemento-enamel junction (CEJ) area and the root portion of the central incisor come to lie mesial to the unerupted lateral incisor crowns. This leads to the fairly rapid provision of space at this level in the alveolus [12]. The lateral incisor migrates labially into this area as it begins its downward eruption path. Additionally, the downward eruption movement distances it from the permanent canine crown, providing more space for it to move labially, following closely after the central incisor.
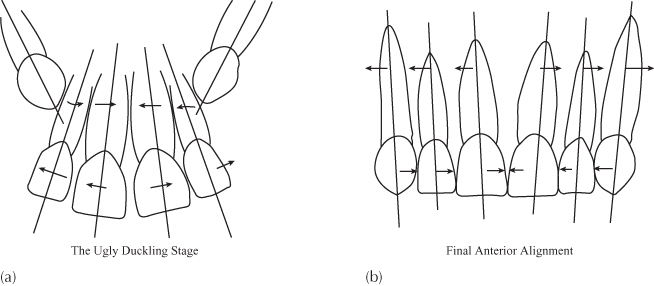
With the eruption of the central incisors, the lateral incisor crowns move from a lingual relationship into a direct distal relationship with the central incisor roots, initially at a higher level (Figure 6.2c). As this occurs, the presence of the lateral incisor crowns displaces the developing roots of the central incisors towards one another, since these are at the same level within the alveolar bone. With the central incisor apices held together in this way, the crowns of these teeth are flared distally. A developmentally normal median diastema is thus produced, which has been termed the ‘ugly duckling’ [13].
A year or so later, the lateral incisors will have descended along the distal side of the central incisor roots, to release their ‘hold’ on the narrowed inter-radicular width of the central incisor roots, allowing the roots to drift apart. The lateral incisors continue to move inferiorly along their eruptive path, progressively reducing their constricting influence on the central incisor roots until they reach the distal side of the necks of the central incisor crowns. At this point, their presence and continued downward migration serve to provide a mesially directed force to the crowns of these teeth, moving them towards one another and partially closing off the median diastema. The long axes of the central incisor teeth will also have changed, with the roots becoming more parallel. The lateral incisor long axes, however, are relatively flared in the coronal direction, with their root apices close to those of the central incisors.
A periapical view of the area at this time will show the unerupted permanent canine crowns of each side pointing mesially towards the lateral incisor apical area. They appear to be the containing influence that causes the apical convergence of the incisor roots and the reason that the median diastema has not completely closed. Subsequent follow-up radiographs of the area will show the permanent canines altering their relationship as they move downwards along the distal side of the root of the lateral incisors. Having initially constricted the roots of the lateral incisors mesially, the downward descent of the canines alters their influence on the lateral incisor crowns, to tip them mesially. This brings about an uprighting of the long axes of the incisors on each side and a closure of the anterior spacing (Figure 6.3). The canines’ own long axes become more vertical as they progress and as the roots of the deciduous canines become resorbed. With the shedding of the deciduous canines, they finally erupt with a slight mesial inclination, taking up their place in the arch by moving the crowns of the incisors towards the midline, to close off the diastema completely [14]. As all this occurs, the long axes of the incisor teeth change from being apically convergent to become more parallel and even slightly divergent.
Fig. 6.3 (a) In the early stages the unerupted canines are mesially directed, restricting the incisor roots to the area of the midline, thereby flaring their crowns distally, to create spacing. (b) As the canines descend towards the crown, down the distal aspects of the lateral incisor roots, their influence is reversed. They now apply a mesially directed force on the distal surfaces of the lateral incisor crowns, which closes off the anterior spaces and encourages a distal root flaring.
Throughout the period of their downward progress, the permanent canines are conspicuously palpable on the buccal side of the alveolar ridge, from as early as 2 or 3 years prior to their normal eruption, which normally occurs at the age of 11–13 years.
Theories Regarding the Causes of Palatal Displacement
Long Path of Eruption
From the days of Broadbent, in the 1940s, the most common reason given for palatal displacement of the permanent maxillary canine was the fact that it had a long and tortuous eruption path, beginning close to the floor of the orbit. It was considered that, compared with other permanent teeth, this tooth had much further to travel before it erupted into the mouth and that it therefore had a greater chance of ‘losing its way’. This has been standard teaching for many decades.
Crowding
Hitchin [15] considered that crowding of the dentition was the reason for this condition, although he offered no evidence to support his contention.
In general, crowding of the dentition results in the exaggerated displacement of a tooth from its developmental position in the arch. The developmental position of the maxillary lateral incisor is lingual to the line of the arch, as we have described above. Thus, when crowding affects the early mixed dentition, there will be insufficient space for the lateral incisor to migrate labially between the root of the erupting or newly erupted central incisor and the deciduous canine teeth, which is the manner in which it normally comes into the dental arch. For the most part, therefore, it continues to develop downwards, but in a lingual position, and erupts lingual to the adjacent teeth.
A parallel environment is created when a second deciduous maxillary molar is extracted before its due time and the first permanent molar drifts mesially into the available space. Similarly to the lateral incisor, the developing second premolar develops palatally to the line of the arch, and its continued development and eruptive path will be in an exaggerated palatal direction in much the same way.
We have pointed out above that the normal eruption path of the permanent canine is buccal to the line of the arch, and we also know that the lateral incisor and first premolar, the teeth immediately adjacent to the canine, erupt before the canine. Thus, in the presence of crowding, there will be reduced space in the arch in the canine area and the close proximity of these adjacent teeth will prevent the canine from moving into the arch. The vertical development of the maxillary permanent canine will therefore be accompanied by its buccal displacement, to give the typical picture seen in the class 1 crowded case (Figure 6.4). Whether the tooth eventually erupts or remains impacted is irrelevant, although buccal impaction is uncommon in Caucasian population groups. It is therefore quite clear that the cause of this type of displacement of the canine is completely different from that involved with palatal displacement. The two conditions are different entities. They should never be confused, nor should they be lumped together to form an experimental group for clinical research, as if to offer a homogeneous sample of impacted teeth. For the purposes of study, it is far more logical to combine all palatally displaced canines, whether they are unerupted or erupted, since they share a common aetiology, although their clinical presentation may be different.
Fig. 6.4 Buccally displaced maxillary canines due to a crowded arch.

In a series of clinical research studies, Jacoby [16], Becker [17] and Brin et al. [5] pointed out that the likelihood of palatal displacement is much reduced where crowding is present. They have shown it to be a far more prevalent occurrence when there is excessive space in the dental arch.
Non-Resorption of the Root of the Deciduous Canine
Lappin [18] considered that it is the failure of the root of the deciduous canine to resorb that causes a palatal deflection of the eruption path of the permanent canine, leading to its impaction. Here, too, one may draw a parallel with other teeth. In cases where a second deciduous molar is over-retained, owing to the presence of a malposed premolar tooth germ, one may often see on the periapical or panoramic radiograph that one of the roots has totally resorbed, while the second root is only partially so. The long spicule of unresorbed root that may be present retains the tooth against natural shedding, while the fully developed and unerupted second premolar is situated immediately beneath the crown of the deciduous tooth in the area previously occupied by the resorbed portion of the roots.
From this type of clinical evidence, which is seen so widely and frequently in practice, it is generally considered that the presence and advancing eruption of the permanent tooth provides the stimulus for the resorption, and a portion of root distant from the unerupted permanent tooth may be unaffected by this process. On the basis of this, Lappin’s view would appear to be ‘putting the cart before the horse’. Nevertheless, and in support of his argument, subsequent studies [19–22] have shown the spontaneous eruption of previously impacted canines in many cases, following the extraction of deciduous canines. This will be discussed at length later in this chapter, under the heading ‘Preventive treatment and its timing’.
Trauma
In a clinical report, Brin et al. [23] have illustrated how trauma, which leads to a cessation in the development of a lateral incisor root, may be associated with palatal canine impaction. They explain this by assuming:
- that the traumatic episode may have caused movement of the lateral incisor, or
- by conduction, movement of the unerupted canine itself, or
- in terms of the guidance theory, that this could be explained as being due to the shortness of the lateral incisor root, whose development ceased as a result of the trauma.
Soft Tissue Pathology
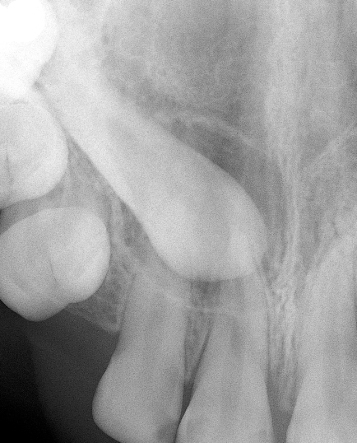
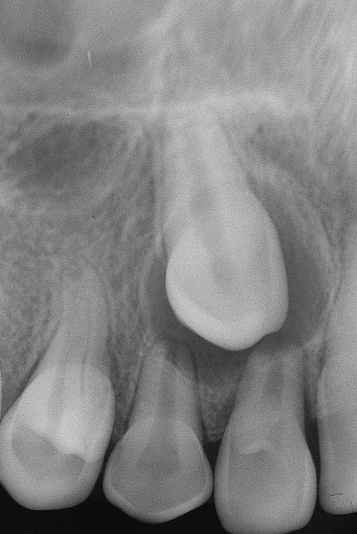
A further alternative could place the blame on the possible presence of chronic irritation, residual infection or granuloma around the apex of a non-vital deciduous canine tooth (Figure 6.5). Deciduous maxillary canines may often be affected by interproximal, usually distal, caries. The lesions are frequently left untreated in the belief that the teeth are about to be shed. The tooth loses its vitality when caries reaches the pulp and a chronic periapical area develops. This soft tissue lesion by itself is a potent cause for deflection of the path of a developing unerupted maxillary canine (Figure 6.6). In rare instances, it may develop into a radicular cyst or it may initiate cystic change in the follicle of the canine, either of which will alter the path of eruption of the canine, or prevent its further eruptive progress. This will be discussed in Chapter 11.
Fig. 6.5 (a, b) Periapical views of bilaterally impacted canines, each associated with a non-vital deciduous canine.
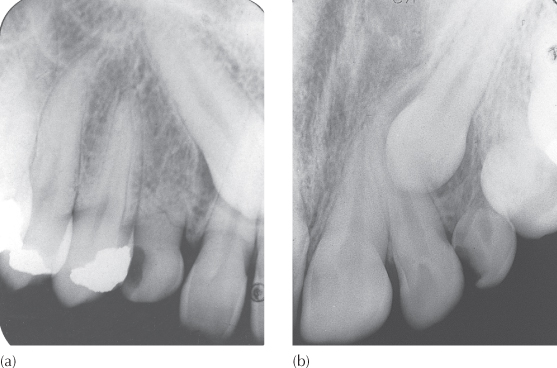
Fig. 6.6 (a) Panoramic view of a patient in the mixed dentition stage with a markedly displaced and unerupted right maxillary canine. The immediate area shows a large area of bone loss involving the canine and first premolar, associated with the non-vital deciduous first molar. The chronic periapical abscess represents a soft tissue obstruction that has deflected the eruption path of the permanent canine. The deciduous canine has an obliterated pulp. (b) Following extraction of the deciduous canine and deciduous first molar, there has been spontaneous resolution, with eruption of the teeth. For no apparent reason, the deciduous canine of the opposite side was overlooked!
(Courtesy of Dr A. Renert.)
The Guidance Theory
Miller [24] and Bass [25] reported that there appeared to be an unusually high prevalence of congenitally missing lateral incisors associated with palatally impacted canine teeth. They theorized that, under these circumstances, the permanent canine lacks the guidance normally afforded by the distal aspect of the lateral incisor root. As pointed out earlier, in relation to normal development, the canine initially has a strong mesial developmental path, which alters early on, with the canine being guided downwards, apparently along the distal aspect of the lateral incisor root. They concluded that, in the absence of this guiding influence, the canine continues in its initial mesial and palatal path. The tooth then becomes impacted in the palatal area, posterior to the central incisors, and fails to erupt in its due time, if at all.
Miller’s concept was founded on information gleaned from the study of six such cases. He assumed that since a peg-shaped or otherwise abnormally small lateral incisor develops a root of more or less normal length, such a tooth would provide the required guidance for the normal eruption of its adjacent canine. He therefore rationalized that these anomalous teeth could not be an aetiological factor in canine impaction.
Following the treatment of several hundred cases of this type by the present author, a different pattern of association seemed apparent. Palatal impaction of the maxillary canine appeared to be intimately bound up with the occurrence of anomalous lateral incisors and less with the congenitally missing teeth. Furthermore, a stereotype of the maxillary impacted canine patient could be offered (Figure 6.7), in which the patient is frequently a 15-year-old female, with well-aligned and normally related dental arches, slight spacing and no real malocclusion. Characteristically, the teeth are small, the lateral incisors particularly so, the incisors lack their normal rounded contour, there may be missing teeth, dental development is late and the patient’s motivation for treatment is low.
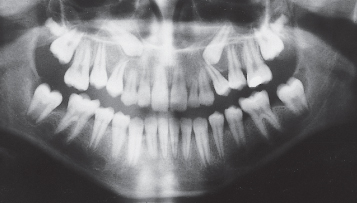
Fig. 6.7 Late-developing dentition showing spacing, small peg-shaped lateral incisors, teeth of poor anatomic contour and minor class 1 malocclusion.

A series of clinical research studies followed, in which a sample of patients who were successfully treated for a palatally displaced canine was investigated. In the first study [10] a wide and highly significant discrepancy in the numbers of normal, small and peg-shaped lateral incisors adjacent to an affected canine was found, compared with the published data for normal populations (Figure 6.8). In the interests of accuracy, a random study was later performed by the same research group [5] to quantify the various types of lateral incisors found within the general population of the same geographic area, while using the same definitions of anomaly. In the general population, 93% of all lateral incisor teeth were of normal shape and size, compared with only 52% in the palatal canine sample. In the random population sample, missing lateral incisors were found in approximately 1.8% of the cases [26], which contrasted markedly with the 5.5% of this anomaly among the impacted canine cases [10] or three times as frequent (Figure 6.8). These figures are valid for the Israeli population sample studied. However, congenital absence of maxillary lateral incisors in a meta-analysis of the collected data from a large number of different population studies was found to be lower, at 1.55% for males and 1.78% for females [27].
Fig. 6.8 Lateral incisor anomaly in patients with palatally displaced canines.
From ref. [5], with permission.
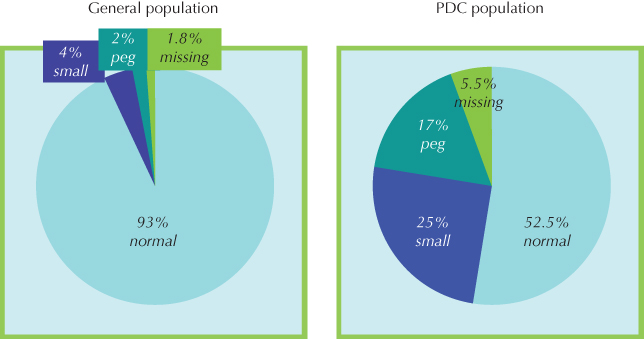
These results clearly support Miller and Bass regarding the part played by the lateral incisor as a guide in the normal eruption of the permanent canine. Without this guidance, normal eruption is compromised fivefold. However, Miller’s rationalization regarding the positive role of anomalous lateral incisors appears very much misplaced. Small lateral incisors were seen in only 4% of the random sample, while the palatal canine cases showed this anomaly to be six times as frequent (25%). Furthermore, only 2% of the general population had peg-shaped incisors, while 17% (nine times the frequency) were seen among the palatal canine cases. Similar results have since been shown in confirmatory studies that have examined Welsh [9] and west of Scotland [28] samples. If small or peg-shaped lateral incisors provide similar conditions to normally shaped lateral incisors in their role in the normal eruption of the canines, then one would expect figures for the association of these anomalous teeth with palatal canines to be much lower than the 5.5% figure for missing lateral incisors. Their presence is shown here to offer more than merely a loss of guidance to the developing permanent canine. The fact that they are associated with a greater prevalence of impaction compared to that of the missing lateral suggests that an additional, obstructive role is played by these teeth.
In the first study [10] a hypothesis was presented based on the fact that the anomalous small and peg-shaped lateral incisors develop very much later than normal lateral incisors. While no figures are available for the extent of this delay, it seems clear from clinical observation that it may be as much as three years – and this for teeth whose calcification normally begins at age 10–12 months!
If we are now to relate this to the ‘guidance theory of impaction’, we may postulate that at the critical time that the permanent canine requires the guidance, the root of the anomalous lateral incisor is too rudimentarily developed to provide it. Thus, initially the situation is parallel to that seen in congenital lateral incisor absence. The result is that the canine develops mesially and palatally and usually in a downwards direction, into the vertical alveolar process, where it proceeds towards the palatal periosteum. This describes the first stage of palatal displacement.
The palatal periosteum may then halt further progress of the tooth, or it may alter the eruption path to a more horizontal direction, across the palate. In either instance, this may then be defined as a first-stage palatal impaction.
In particular circumstances, it seems that the palatal periosteum may deflect the developing canine from its first-stage displacement, in a downward direction. The alveolar process in the canine region is V-shaped in cross-section, such that, with continued vertical movement, the progressively narrowing alveolus will tend to guide the aberrant canine in a buccal/labial direction. These corrective movements of the palatally displaced canine are the characteristic feature of what may be termed the first stage of palatal displacement with secondary correction (Figure 6.9).
Fig. 6.9 (a–c) Serial radiographs showing the relationship of an unerupted canine to a late-developing and peg-shaped lateral incisor. (d) The two teeth have erupted and are superimposed on one another. At clinical examination the erupted canine was found to be on the palatal side of the lateral incisor.
In cases of congenital absence of the lateral incisor, a canine that was not palpable buccally at any point in its earlier development may often be seen to finally erupt more mesially than normal and in the line of the arch. In the presence of an over-retained deciduous lateral incisor or canine only, the corrective movements of the canine lead to the initiation of root resorption of these deciduous teeth. Following their shedding, the permanent canine may then erupt into the line of the arch and, often, in a more mesial location in the place of the absent lateral incisor. If a late-developing lateral incisor is present, it will now lie directly in the path of the displaced canine. The physical presence of the lateral incisor will bring an abrupt stop to these corrective movements, and any further vertical development of the canine may only then be on the palatal side of the dental arch, completing the second stage of palatal displacement. In summary, therefore, the ‘guidance theory’ comprises five elements:
1. Normal eruption. It adopts Broadbent’s original view that, given the timely and normal development of a lateral incisor, guidance for the canine is provided by the presence of a normally developing lateral incisor and a buccal path of eruption is to be expected, with the tooth palpable in the buccal sulcus early on.
2. First-stage impaction. It offers an explanation for the absence of guidance at a critical time in the normal development of the permanent canine, which leads to a deflection of the developmental path of the tooth, causing it to move palatally. This etiologic factor may be created by a congenitally missing lateral incisor or by a late-developing, anomalous lateral incisor. In the event that no vertical movement of the canine into the alveolar process occurs, the result may be a horizontal palatal impaction.
3. First-stage impaction with secondary correction. It goes on to explain the corrective influence of the vertical alveolar process, which redirects the canine on a more favourable downward path. This scenario may be difficult to diagnose accurately, and the clinician must draw his or her own conclusions from the further progress of the impacted tooth, which may be palpable, low down on the palatal side, before it finally erupts close to the line of the arch. The tooth may then spontaneously move more buccally and mesially, in the absence of a lateral incisor, to reach the occlusal plane in a close-to-normal bucco-lingual position.
4. Second-stage impaction. Self-correction is prevented by the presence of an anomalous and late-developing lateral incisor, redeflecting the tooth further palatally. This may be termed second-stage displacement, and is an aetiological factor that is not seen when the lateral incisor is absent.
5. Second-stage impaction with secondary correction. As we shall see later, in the discussion of treatment timing, extraction of an over-retained deciduous canine, or even the anomalous lateral incisor itself, may often lead to spontaneous eruption of the impacted tooth.
There are several elements in this process which clearly indicate that the erupting canine is strongly influenced in the progress of its eruptive movements by environmental conditions, which determine the degree of success of its final eruption status, including its final erupted location, or its impaction. Small, peg-shaped, and missing teeth are more frequent findings among females than among males, in the approximate ratio of 2–3:1, as discussed earlier in this chapter. Furthermore, the maxillary permanent canine erupts earlier in females, which could mean that earlier lateral incisor guidance will be necessary for its normal eruption. These facts provide the hypothesis with some support in explaining why palatal canines are more frequent in females and why anomalous lateral incisors are a more powerful causal agent than congenitally absent lateral incisors.
It is quite clear that heredity plays an important role in this hypothesis. The assumption is that the genetically determined factors (small, peg-shaped, missing lateral incisors, spaced dentitions, etc.) provide the environment that leads to a loss of guidance of the canine, its abnormal palatal path, and impaction.
Heredity
Given the strong hereditary influence in palatal canine displacement, there are those who believe that heredity is the direct cause and dismiss other relationships as secondary or as similarly linked hereditary factors. In other words, the palatal canine is another link in the chain of genetically linked phenomena.
In a study of the families of children affected by palatally displaced maxillary canines [29] a search was made among the parents and the siblings for the related anomalies to which we have referred above. The prevalence of small, peg-shaped and missing lateral incisors, late-developing dentitions and other missing teeth among these close relatives was very high, in addition to palatally impacted canines. This evidence seems to favour heredity as the causal agent for these associated phenomena. The guidance theory contends that their presence creates an environment favourable to the development of palatally displaced canines and, as was to be expected, the lateral incisor phenomena were found to occur in an unusually high proportion of these cases. The view that these phenomena are each genetically determined and frequently occur together, including the canine displacement [30–32], is equally tenable, but would appear to be an oversimplification. The fact that the extraction of adjacent deciduous canines and anomalous lateral incisors and orthodontic space opening greatly improve the chances of canine eruption would lead us to believe that local factors cannot be ignored as exerting a powerful influence on the aetiology of canine impaction.
Other forms of maxillary canine positional anomaly do occur from time to time, and are difficult to equate with the more usual pattern of palatal or buccal displacement. Genetic factors seem likely to be the governing factors, in which the entire tooth is located in an abnormal position. In these cases, it seems that the original site or orientation of the anlage from which the tooth developed was abnormal. Thus, we occasionally come across patients in whom there is adequate space in the arch for the ideal eruption and alignment of the maxillary permanent canines, yet these teeth erupt buccally ectopic (Figures 6.10 and 6.11). Additionally, the eruption occurs relatively high in the alveolus and the tooth has no mesio-distal contact with its immediate neighbours and, therefore, cannot be considered to have been guided into this position.
Fig. 6.10 Maxillary canine/first premolar transposition. An example of hereditary primary tooth germ displacement.

Fig. 6.11 Despite the absence of crowding, the canine has erupted in an abnormal location. Is this evidence of a lack of guidance on the part of the adjacent peg-shaped lateral incisor or hereditary primary tooth displacement?

On the other hand, this may be looked at and perhaps explained in the parlance and context of the guidance theory. As we have illustrated above, buccally displaced canines (BDC) are usually found in crowded dentitions. Nevertheless, there is a small but significant percentage of BDC cases where there is no crowding to account for the buccal displacement. A study was undertaken by the Jerusalem group to investigate the features of dentitions of BDC cases where no crowding was present and compared them with BDC cases with crowding and cases in which the canines had erupted normally. The results revealed reduced dimensions of the maxillary incisors in BDC in dentitions in which no crowding existed in comparison to the other two groups. More specifically, the lateral incisor was the only tooth which was consistently smaller when compared to both crowded BDC and normally erupted canine cases [33]. As pointed out earlier in this chapter, small lateral incisors develop very late, growing adequate root length at a time which is too late for it to influence the developing canine. Thus, it may be reasonably postulated that the lack of guidance from the anomalous adjacent lateral incisor provides a cogent alternative explanation for the buccal displacement of the canines in non-crowded dentitions, in a similar way to what occurs in the palatally displaced canine cases. The canine simply takes a buccal path instead.
It becomes clear from a careful reading of this section that there are both undeniable hereditary and environmental/developmental factors at work in the aetiology of maxillary canine impaction, neither of which may be discounted and both influencing the expression of the aberrant eruption. For a balanced, updated, evaluative and critical discourse on the place of both these elements as causative agents, the reader is referred to a recently published review (34).
Peck et al. [35] have studied maxillary permanent canine/first premolar transposition (Figure 6.11), and have found a strong hereditary influence in its aetiology. They point out that this very specific type of canine anomaly cannot be construed as deriving from guidance from the lateral incisor, and cannot be influenced in any way by the size, form or timing of the development of that tooth. With somewhat questionable justification, they then extend their reasoning to cover all maxillary canine displacements. They go on to claim that their findings, specifically vis-à-vis transposed canines, represent conclusive evidence that the aetiology of palatal impaction is also under total genetic control (Figure 6.12).
Fig. 6.12 A case of bilateral hereditary primary tooth germ displacement.
Canine/first premolar transposition and palatal displacement of the canine are both aberrations of tooth position, but there is no reason for assuming that the aetiology of the one is the same as for the other, and there can be no basis for comparing transposition with palatal displacement. This does not, therefore, present a valid argument with which to refute the ‘guidance theory’ [36].
We may prefer to define canine/first premolar transposition as primary tooth germ displacement [37]. In other words, their site of development is not in its expected location in the jaw and in relation to the other teeth. In the developed dentition, this is reflected in an abnormal position of the root apex, which is usually assessed clinically by the mental exercise of extending the orientation of the long axis of the tooth crown. This helps us to distinguish them from other and more common forms of displacement, which have an environmentally influenced aetiology.
As a result of crowding, the position of the more frequent buccally placed canine is dictated by the amount of space available for it in the arch and by direct interproximal contacts with the adjacent teeth. The vast majority of buccally and palatally displaced canines show the root apex to be ideally placed, in the line of the arch [36]. Experience shows that extrusion and tipping of the crown into its place in the arch is usually sufficient to resolve the malalignment, with little or no root torque being required in most cases.
Other Associated Clinical Features
Repeated studies have found that palatal canine patients have dentitions characterized by their small teeth [5, 10, 16, 35, 36]. In the general population, the individual teeth of males are larger than those of females, but a study of patients with palatal canines discovered that the individual teeth in the affected males were found to be significantly smaller than in unaffected males [38]. However, there was no difference in the size of teeth between affected and unaffected females. Oddly, the teeth of affected males were similarly sized to those of affected and unaffected (control) groups of females.
Both male and female patients with palatal canines often feature missing teeth, such as third molars, maxillary lateral incisors, mandibular and maxillary second premolars, and mandibular central incisors [5, 7, 24, 25, 30, 33, 34].
From the literature, we learn that small and missing teeth in a dentition have been shown to be associated with late development [39–41], a fact that has largely escaped attention. Scant notice was taken within the profession of the shrewd observation made by Newcomb half a century ago [41] that ‘with few exceptions … potential impaction of permanent teeth is seen in patients exhibiting moderate to severe retardation of dental maturation … [and] … a slow rate of permanent teeth formation’. He considered ‘it would be useful … to correlate dental and bone ages’ among these patients. Newcomb based his conclusions on dental age as determined by the eruption status of the dentition. However, no specific study was ever undertaken to investigate this connection until recently.
In a more recent study that attempted to investigate this factor, the 55 cases with palatal canines which constituted the experimental group were assessed for dental age on the basis of the root development of the dentition, as seen on the radiographs and using the principles outlined in Chapter 1. This is a more accurate method of age assessment than eruption status, which may be influenced by local factors. In approximately half of the cases, development was seen to be in line with the norms for their ages, while in the remainder, significant developmental delay was seen. None of the affected cases showed advanced dental development, underlining the absence of a normal distribution for dental development and a strong tendency for lateness [42].
As seen in the discussion in relation to tooth size, a sexual dimorphism in the pattern of delayed dental development was found. A dental age significantly younger than the chronological age was noted among affected males more than twice as frequently than among affected females. In the males, late dental development was observed in half the individuals with palatal canines, which was accompanied by the presence of smaller than average teeth and a high frequency of lateral incisor anomaly. The other half of the males showed a timely developed dentition, a statistically non-significant increase in the incidence of lateral incisor anomaly, and mesio-distal width reduction only in the maxillary central incisors and first molars. This latter male sub-group therefore resembled the unaffected cases that made up the control group in this study. Among the females, late dental age was accompanied by a slight increase in lateral incisor anomaly, although overall tooth size was not affected. With such contrasting and partially conflicting findings regarding tooth size and retarded dental development seen in males and females who exhibit palatally displaced maxillary canines, investigations of tooth size, congenital absence and dental age which involve a combined male–female group of patients, will produce confusing results. This combination may obscure important differences that exist between the sexes.
Infra-occluded deciduous mandibular molars have also been found in larger numbers in cases with palatal canines [7, 42]. The explanation may be viewed from the same two distinct standpoints. The first assumes that the canine aberration is totally hereditary and is linked with the associated hereditary factors of lateral incisor anomaly, late dental development, small and missing teeth – to which it is now proposed to add infra-occluded deciduous molars as an additional hereditary factor. The alternative standpoint notes that over-retained and infra-occluded deciduous molars are often found in situations where their permanent successors are small or congenitally absent. In both these situations, resorption of the roots of the deciduous molars may be partial, sometimes involving only one of the widely divergent roots. This results in over-retention of the deciduous molar and, under these circumstances, it is more likely to become infra-occluded than one that sheds normally and in its due time. Dentitions with small or missing premolars are often associated with lateral incisor anomalies, which have been shown to be allied with palatal canines, as we have discussed earlier in this chapter. Thus, the association between infra-occluded mandibular molars and palatal canines is an indirect one, with linked hereditary factors bringing about changes elsewhere, which generate the guidance factor that causes the canine aberration.
There are more compelling arguments that seem to favour the guidance theory. For around half a century, it has been accepted that small and peg-shaped incisors represent a weak or partial expression (incomplete penetrance or microform) of congenital absence [43–48]. It follows, therefore, that if palatal displacement of a maxillary canine is under hereditary control, then one would expect to see this form of ectopia more frequently associated with congenital absence of the adjacent lateral incisor than with a lateral incisor of reduced size. Not only does this not occur, but the reverse appears to be true, with a significantly higher proportion of palatal canines involved with lateral incisors of reduced size [9, 10, 28, 36, 42].
In order to confirm or negate this reported tendency and to provide a firm scientific base for this apparent paradox, a study was designed in which the sample consisted of patients who were taken serially from the files of the Orthodontic Departments in the Universities of Jerusalem and Tel Aviv and in orthodontic private practice in Israel [49]. From a patient base of approximately 12 000 consecutively treated patients, only those exhibiting an anterior maxilla with the following pre-treatment conditions:
- a missing lateral incisor on one side
- an anomalous (i.e. peg-shaped or reduced) lateral incisor on the other, and
- a unilateral palatally displaced canine
were included in the study. Given such rigorous inclusion criteria, 19 patients remained to form the experimental group. The null hypothesis of the investigation was that if: (a) reduced or peg-shaped lateral incisors are hereditary and represent a microform/incomplete penetrance/partial expression of congenital absence and (b) palatal displacement of maxillary canines is a hereditary condition and associated with the lateral incisor anomaly, then it is logical to assume that the palatally displaced canine will occur far more frequently in association with congenital absence of the lateral incisor than with the dimensionally diminutive tooth. Not only was this not so, but the results of the study showed that in an overwhelming majority of the cases (84%), the palatal canine was found on the side of the anomalous lateral incisor, with only three cases (16%) found on the side of the missing tooth. From this, it was concluded that environmental factors are strongly bound up with the causation of palatal displacement of the maxillary canine and explained in terms of a second stage impaction, as described above.
In the previous chapter, relating to impacted maxillary incisors, we pointed out that an early first phase of treatment is indicated in order to resolve the impaction of the affected tooth. In the long-term follow-up of many of these maxillary incisor impaction cases, it was observed that there seemed to be a substantial number of patients in whom there was a serious disturbance in the eruption of the canine of the same side. Accordingly, a study was undertaken to monitor the further development of children who had been treated for maxillary incisor impaction in the months and years following the resolution of the impaction in their first phase of treatment. Abnormality of position and disturbance of eruption were seen in the canine on the same side as the previously impacted central incisor in 43% of the cases. This was in contrast to the contralateral canine, where the rate of anomaly was only 4.7%. The abnormality in the affected side canine was expressed in several different ways, namely palatal impaction, buccal ectopia and pseudo-transposition with the lateral incisor [50]. The frequent occurrence of canine aberration only on the side where the central incisor had been impacted indicates clear environmental influence (see Figure 6.20). In a radiographic study [51] of a series of 122 Israeli patients with multiple congenitally missing teeth, 20.4% of the maxillary canines were congenitally absent and 42.4% were mesially displaced, of which 5.7% became impacted and mostly adjacent to a missing lateral incisor. Of the remainder, 5.6% were distally displaced and only 26.4% were positioned in their correct locations, mainly adjacent to a lateral incisor. It was concluded that displaced and impacted maxillary canines were very frequently found in this highly special group of patients, although inadequate sample size prevented the drawing of meaningful conclusions.
In summary, it may be learned from all this that the causation of palatal displacement or impaction of the maxillary canine is not due to any single factor. The simultaneously occurring factors related to or causing the canine impaction may be hereditary in nature, such as anomalous or missing lateral incisors, late dentitions and infra-occluded deciduous molars, which themselves are under total genetic control. Equally, however, the path of eruption of the canine may be influenced both favourably and unfavourably by conditions and events that are environmental in nature and include local therapeutic countermeasures, such as orthodontic space opening, prophylactic extraction of the deciduous canine or of a minuscule lateral incisor, or the existence and/or treatment of an adjacent impacted central incisor, or due to a soft tissue lesion or hard tissue body. So, while the aetiological stage may be set by either genetic or environmental factors, there is strong evidence that casts doubt on the simplistic and dogmatic view that the palatal canine itself is solely under genetic control. Unquestionably, maxillary canine eruption is influenced by and responds to altered conditions within its immediate environment. At the time of writing, therefore, ‘there is currently too little robust statistical or genetic evidence to definitively ascribe malposition of the permanent canine as an isolated disorder of either genetics or environment’ [49, 50].
Complications of the Untreated Impacted Canine
Morbidity of the Deciduous Canine
Early morbidity of the deciduous canine is common for two reasons. First, its root may become markedly resorbed, even when its unerupted successor is quite distant from it, causing considerable mobility and eventual shedding without the possibility of replacement by the permanent tooth. This creates a problem in terms of restoration, since the space is usually too small for a satisfactory replacement either by the misplaced permanent canine or by some form of artificial fixed bridge pontic or implant.
The second reason that such a tooth may not survive relates to its relatively high susceptibility to interproximal (particularly distal) caries. As we have pointed out, it is still common to see a fairly extensive distal cavity in this tooth at around the age of 11 or 12 onwards, which may have been deliberately left untreated by a general practitioner who was unaware of the likelihood or existence of impaction of its permanent successor.
Cystic Change
Loss of vitality may occur very early on in the carious process in the deciduous canine teeth, owing to the narrow width of the hard structures of these teeth and the relatively large pulp. Necrosis of the pulp and periapical pathology may then be asymptomatic. Under these circumstances, there may be a direct interconnection between the apical pathology and the follicular sac surrounding the impacted canine. This may stimulate an enlargement of the follicular sac, which is clearly seen on a periapical radiograph. It may also undergo cystic change, to produce a dentigerous cyst (Figure 6.13). This may also occur without any relation to pathosis of the deciduous canine. In strictly radiological terms, an enlargement of the follicular sac to beyond 2 or 3 mm is generally considered to represent cystic change. In rare cases, these cysts may expand at the expense of surrounding maxillary bone and displace the canine higher and higher in the maxilla. Alternatively, the chronic periapical lesion on the deciduous canine may itself become cystic – a radicular cyst – and its subsequent enlargement may displace the adjacent teeth, including the palatal canine. The subject of cysts in relation to impacted teeth will be described separately in Chapter 11.
Fig. 6.13 A dentigerous cyst surrounds the crown of an impacted canine.
Crown Resorption
The reduced enamel epithelium surrounding the completed crown of a tooth separates the crown of the tooth from the surrounding tissues. This intact epithelial covering may degenerate with age if the tooth remains unerupted, and its integrity may be lost. This allows bone and connective tissue to come into direct contact with the crown of the tooth. In time, osteoclastic activity will lead to resorption of the enamel and its replacement by bone – a process known as replacement resorption. Over a long period, repeated radiographs of the tooth will show a poorer definition of the profile of the crown, with the enamel becoming less and less contrasting in its opacity, highlighting this bone-for-enamel substitution (Figure 6.14). Subsequent surgical exposure of the crown of this tooth will show a pitted surface, which is difficult to separate from the surrounding bone, and sparse soft tissues.
Fig. 6.14 Periapical view of maxillary incisor area in a 63-year-old female, showing advanced replacement resorption of the crowns of two impacted canines. The follicles of both teeth are almost completely absent and the teeth are very radiolucent, with poor definition.

This condition seems more likely to occur in adult patients in whom the impaction has been left untreated over two or three decades [52] and is almost certainly the reason why, when attempting treatment of impacted teeth in adults in the fourth or fifth decade of life, the chances that the tooth will not respond to orthodontic force may be high [53].
Resorption of the Roots of the Incisors
The proximity of the follicular sac of an unerupted permanent tooth to the roots of its deciduous predecessor appears to be the trigger that initiates the process of root resorption, probably as the result of pressure. The progress of this resorption process is then maintained by the further advance of the eruption of the permanent tooth, which moves into new areas vacated by the resorbing root. This is part of the normal process of transition from the deciduous to the permanent dentition.
Little is known about the reasons for the resorption of the roots of deciduous teeth that leads to their eventual shedding and why this does not normally occur with the roots of permanent teeth. Histologically, there is no way to tell the difference between the root tissue of a deciduous and that of a permanent tooth. Under certain conditions, however, the presence of an unerupted permanent canine tooth may be associated with the resorption of the root of the adjacent lateral (Figure 6.15) or central incisor [53–59]. Furthermore, and in a manner similar to that seen with deciduous teeth, the progress of this undesirable phenomenon depends on further eruptive movements on the part of the impacted tooth.
Fig. 6.15 The impacted canine crown is surrounded by a large dentigerous cyst, with associated root resorption of both the deciduous canine (to be expected) and the permanent lateral incisor (pathological).
In this context, it is perhaps pertinent to comment that the maxillary canine and, occasionally, the third molars are almost the only permanent teeth whose eruptive movements, both successful and unsuccessful, may cause resorption of the roots of neighbouring teeth to any significant degree. They are also the only permanent teeth that normally develop in close relationship with the developing apical areas of the roots of other permanent teeth, while the premolar teeth develop in a restricted area, encompassed by the roots of the deciduous molars and at a distance from other permanent teeth. However, in rare instances an aberrant and deeply located second premolar may cause the resorption of the mesial root of the first molar (see Figure 7.2). The central incisors and first molars erupt before their adjacent neighbours, and the lateral incisor is related to the neck area of the crown of the central incisor. The canine, however, is closely related to the roots of the adjacent lateral incisor and first premolar, while it is still fairly high in the maxilla during most of its eruption period. Similarly, unerupted third molars in crowded positions in the ramus or tuberosity areas may come into close relation with the root portion of the second molars, where similar damage may occur.
Diagnosis
Unerupted permanent maxillary canines cause the patient relatively few problems, unlike impacted mandibular third molars. A retained deciduous canine may have a relatively poor appearance compared with a properly aligned permanent canine, but most patients are frequently unaware of the presence of and do not seek treatment for the over-retained deciduous canine. The discovery of palatal impaction is therefore usually made by the general dentist during routine dental examination.
Inspection
The maxillary permanent canine normally erupts at a dental age of about 11 years. Its non-appearance at this age should invite clinical inspection and radiographic investigation, especially if its antimere is present.
The maxillary incisor teeth are normally spaced and flared laterally until the age of 10 years, as described earlier in this chapter. Should this situation still be true by 11 or 12 years, the clinician should be suspicious, since this means that there is a detail missing from the mechanism that smoothly transfers Broadbent’s ugly duckling stage into the final adult alignment, with interproximal incisor contacts. Indeed, a resultant persistent median diastema may be the factor that brings the patient to the office to request treatment, unaware of the impacted canine.
It is unlikely that a missing lateral incisor or a frankly peg-shaped incisor will be overlooked. Nevertheless, care should be taken to examine the size and shape of existing lateral incisors. Central and lateral incisors whose crowns have mesio-distal straight or slightly tapering sides and lack the classical proximal contour are usually small teeth and often develop late. Some of these are frankly peg-shaped, a condition defined by their widest mesio-distal dimension being at the CEJ.
Furthermore, the discovery of a late-developing dentition and a dentition in which there are missing teeth, other than the lateral incisors, should also be treated with a degree of caution. We have reported above that all these factors have been linked with palatally displaced canines, and this possibility should be thoroughly investigated, both at the time when the phenomena are first noticed and in subsequent follow-up examinations that have been scheduled to oversee the smooth changeover from the mixed to the permanent dentition.
Abnormally positioned unerupted canines frequently affect the positions of neighbouring teeth, particularly lateral incisors. We have already pointed out that the root apex of a palatally impacted canine is usually in the line of the arch, with the crown mesially displaced, in addition to its palatal tilt. This brings it into close relation with the palatal side of the lateral incisor, often displacing its root labially. Clinically, this will be identified by the root being very prominent on the labial side of the ridge or by a lingual tilt of the crown of the tooth, sometimes into a cross-bite relationship. In contrast, a lateral incisor whose root orientation indicates a strong palatally directed apical displacement suggests that the unerupted canine is labially placed and, at least to a degree, also somewhat mesially directed (Figure 6.16).
Fig. 6.16 Clues to the position of the unerupted canine. (a, b) The unerupted left canine presents a palpable bulge overlying the root of the lateral incisors, seen from the front and the lateral aspects. At the same time, the lateral incisor root appears to be displaced distally and palatally. (c) From the occlusal view, compared to the orientation of the central incisor, the lateral incisor root has a distinctly palatal axial inclination, which is less obvious in the other two views.

Palpation
We have pointed out above that, under conditions of normal development, the permanent canine is palpable buccally above the deciduous canine for two or three years prior to its eruption. The buccal aspect of the alveolus should be palpated above the attached gingiva and up to the reflection of the oral mucosa. A wide convex contour of the bone is indicative of the canine, immediately beneath. Care should be taken not to confuse this with the narrower profile of the root of the deciduous canine. In the event that this contour is concave, the palatal side of the alveolar process should be palpated to see if there is a clue to its location there. The deciduous canine should always be tested for mobility. If this test is even mildly positive, it will suggest that the permanent canine is fairly close to the desired eruption path and that severe displacement is unlikely. In this situation, the unerupted canine may not be palpable on either side of the alveolar ridge.
When there is a strong palatally directed apical displacement of the root of the lateral incisor, we have just pointed out that it is likely that the canine is also mesially directed. In this case, the unerupted cuspid will usually be palpable high in the labial sulcus and much closer to the central incisor root than to its normal position in the arch, and the contour of the alveolus, superior to the deciduous canine, may be concave. Given the unusual distancing of the permanent canine from its normal position, its deciduous predecessor will have most of its root intact and will consequently exhibit no pre-shedding mobility.
Radiography
As we shall see later in this chapter, to plan the strategy of mechano-therapy properly for a particular case and to obtain a pre-treatment assessment of the periodontal prognosis of the treated result, it is essential to know the exact positions of both the crown and the root apex of the unerupted tooth. A single periapical radiograph is essential to identify pathology, such as root resorption, obstruction and cystic change, but it should be supplemented by other films that will help to precisely locate the unseen tooth.
The use of a second periapical radiograph in the parallax method has the advantage of simplicity of technique and provides both the orthodontist and the surgeon with important information regarding positioning, although the exact locations of crown and apex are difficult to compute from these pictures. A true lateral view (as seen on the lateral cephalogram or on a tangential film) paired with a vertex occlusal or postero-anterior cephalometric view is technically more difficult to obtain, but will provide accurate three-dimensional positional information of the unerupted tooth in its most comprehensible form. However, these films involve a high radiation dosage for a relatively poor return on the amount of information provided.
The central portion of a panoramic radiograph shows the incisor region in the postero-anterior view and will indicate a palatal displacement as an overlap of the impacted canine with the roots of the incisors. This is by far the most popular method used today. The reader is referred to Chapter 2 for a description of how this film may be used by itself, or in combination with a periapical film, with an occlusal film or with a lateral cephalogram, to extract the maximum information regarding the position of an impacted canine.
We have already pointed out that plain film radiography cannot provide reliable information in the bucco-lingual plane and, therefore, incisor root resorption may occur and remain undiagnosed until well advanced. Additionally, the bucco-lingual distance that exists between the impacted tooth and its neighbour is very difficult to assess from these films and this may be an important factor in planning the strategy for the biomechanical resolution of the impaction.
For both these reasons and certainly in relation to all of the more involved cases, it is recommended that the immediate area be subjected to a computerized tomographic examination, using a cone beam volumetric scanning machine, to provide the maximum positional information while, at the same time, reducing the dosage of ionizing radiation to the absolute minimum.
Treatment Timing
In normal circumstances, by the age of 9–10, it is usually possible to palpate a normally developing maxillary permanent canine tooth on the buccal side of the alveolus, high above its deciduous predecessor. In the presence of crowding, and particularly after the eruption of the first premolar, the bulging of the unerupted canine is emphasized. The greater the degree of crowding the greater will be this displacement and the more palpable will the canine become, as its eruptive process brings it further and further down on the facial side of the dental arch. It follows, too, that the greater the buccal displacement the greater the risk that it will erupt through oral mucosa, higher up the alveolar process, rather than through attached gingiva.
In the event that the tooth is not palpable at this age, radiographs should be taken to assist in locating the tooth accurately and to secure other information regarding the presence, size, shape, position and state of development of individual unerupted teeth and any pathology. In a patient younger than 9 years, the radiographs will not usually show abnormality in the position of the unerupted canine teeth, even if the canines are not palpable and even if they are destined subsequently to become palatally displaced. Many of these non-palpable canines will finally erupt into good positions in the dental arch in their due time, provided that there is little or no mesial and palatal displacement of the crown of the unerupted tooth. It may be argued that even canines with an initial mild palatal displacement will achieve spontaneous eruption and alignment despite a first-stage displacement, if they undergo secondary correction (see ‘The guidance theory’ in the section on Aetiology above). Other canines, however, will not erupt, and their positions may worsen in time, as may be seen in follow-up radiographs. If it were possible to distinguish between the two early enough, a line of preventive treatment might be advised.
Preventive Treatment and Its Timing
Using panoramic radiographs of young patients in the mixed dentition, Lindauer et al. [21] were able, to a relatively low degree of reliability (78%) only, to predict palatal impaction on the basis of canine overlap of the root of the lateral incisor.
Extraction as a Means of Prevention: Deciduous Canines
As we indicated earlier in this chapter, several authorities [20, 22] prescribe the extraction of the deciduous canine teeth in an attempt to encourage the permanent canines to erupt. They have recommended seeing the patient and diagnosing the palatal positioning before the age of 11 years, and have shown that extraction performed at this time offers a good prognosis for the natural eruption of the canine, with 78% of the canines in their sample erupting into a clinically correct position. Caution must be advised in interpreting these results, however, since the authors did not study an untreated control group and thus are not in a position to determine just how many of these teeth would have erupted without this preventive treatment [21] (Figures 6.17 and 6.18).
Fig. 6.17 (a) A case diagnosed from this panoramic view as having bilateral palatal canine displacement and referred for extraction of the deciduous canines. (b) A year later, a repeat film shows great improvement in the position of both canines and normal eruption of the canines is imminent, despite the fact that the deciduous canines have not been extracted.
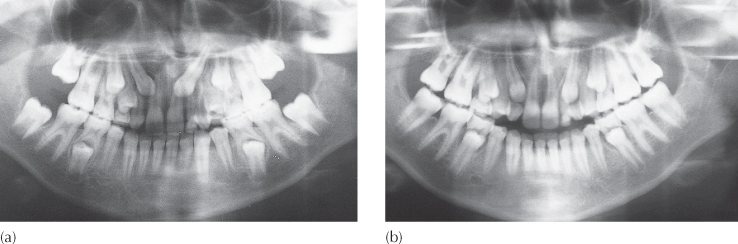
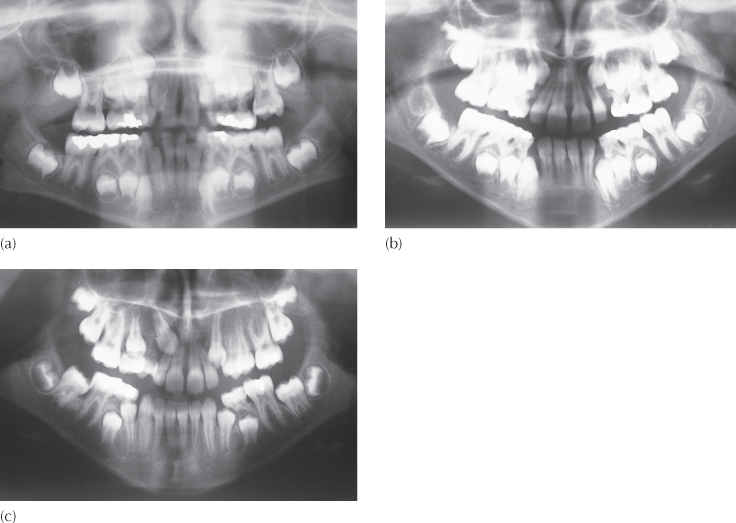
Fig. 6.18 (a) A case of early crowding treated by extraction of four deciduous canines, to relieve crowding at age 8 years. No hint of impending palatal displacement of the canine is discernible on this panoramic film. (b) One year later, the incisors are aligned and spaced. Extraction of the four deciduous first molars (the second stage of serial extraction) was advised. (c) The panoramic view taken a year later reveals the maxillary right canine in a palatally displaced location, despite early extraction of the deciduous canine. Treatment of this case may be seen in Figure 6.41.
From their study, Ericson and Kurol concluded that the prognosis becomes less favourable as the palatally displaced canine’s medial overlap of the lateral incisor root increases and as the angle between the long axis of the canine and the mid-sagittal plane widens. They also noted that, if positional improvement of the canine was not evident within 12 months of the prophylactic extraction, it was unlikely that improvement would occur.
From this discussion and from some considerable anecdotal clinical experience, we may assume that, under certain circumstances, the extraction of a maxillary deciduous canine may be a useful measure in the prevention of incipient canine impaction. To achieve maximum reliability, the following conditions should be met before extraction is advised:
1. The diagnosis of palatal displacement must be made as early as possible.
2. The patient must be in the 10–13-year age range, preferably with a delayed dental age.
3. Accurate identification of the position of the apex should be made and confirmed to be in the line of the arch.
4. Medial overlap of the unerupted canine cusp tip should be less than half-way across the root of the lateral incisor, on the panoramic view.
5. The angulation of the long axis should be less than 55° to the mid-sagittal plane.
4 and 5 on this list represent conditions that, if not fulfilled, may still lead to spontaneous eruption and alignment, so that while the chances are reduced, extraction may still be worth considering.
Notwithstanding, in two studies carried out in Italy by the same researchers, their earlier paper [60] found no statistically significant differences between those cases in which the deciduous canines had been extracted and those in which no extractions were performed. Contradictory figures were presented in their second paper [61], in which deciduous canine extraction produced 65% success against 36% for non-extraction cases.
One further factor that is frequently missed when studying the radiograph and, therefore, not normally taken into account as a causative agent is the occurrence of non-symptomatic soft tissue pathology, specifically chronic periapical abscesses associated with non-vital deciduous teeth and enlarged dental follicles or early dentigerous cysts. These may lead to quite severe displacement and impaction of the unerupted permanent canine. Their elimination may often have a favourable outcome even when displacement is quite extreme (Figure 6.6). The reader is referred to Chapter 11 for a description of the treatment of teeth impacted in positions of extreme displacement by dentigerous cysts.
Given that there is no truly reliable method of early detection of a potential palatal displacement [21], a claim that it was the pre-emptive extraction of the deciduous canine that had elicited the normal eruption of a permanent canine must be viewed with some reservation on the basis of the present state of our knowledge. Clinical experience would lead us to be encouraged by the procedure in many cases, but an accurate assessment of its efficacy has still to be determined.
In the mixed dentition period, the unerupted maxillary canine is often held too far mesially by the mesio-distally wide crown of the unerupted first premolar immediately distal to it. If clinical experience is to be countenanced in these days of evidence-based treatment decisions, the author has found that, together with the extraction of the deciduous canine, there is merit in the simultaneous extraction of />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


